Extracorporeal Membrane Oxygenation for Acute Respiratory Distress Syndrome following HAART Initiation in an HIV-infected Patient Being Treated for Severe Pneumocystis jirovecii Pneumonia: Case Report and Literature Review
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Hanyang University Hospital, Seoul, Korea. paihj@hanyang.ac.kr
- KMID: 2350926
- DOI: http://doi.org/10.4266/kjccm.2016.31.2.162
Abstract
- Pnuemocystis jirovecii pneumonia (PJP) is one of leading causes of acute respiratory failure in patients infected with human immunodeficiency virus (HIV), and the mortality rate remains high in mechanically ventilated HIV patients with PJP. There are several reported cases who received extracorporeal membrane oxygenation (ECMO) treatment for respiratory failure associated with severe PJP in HIV-infected patients. We report a patient who was newly diagnosed with HIV and PJP whose condition worsened after highly active antiretroviral therapy (HAART) initiation and progressed to acute respiratory distress syndrome requiring veno-venous ECMO. The patient recovered from PJP and is undergoing treatment with HAART. ECMO support can be an effective life-saving salvage therapy for acute respiratory failure refractory to mechanical ventilation following HAART in HIV-infected patients with severe PJP.
MeSH Terms
Figure
-
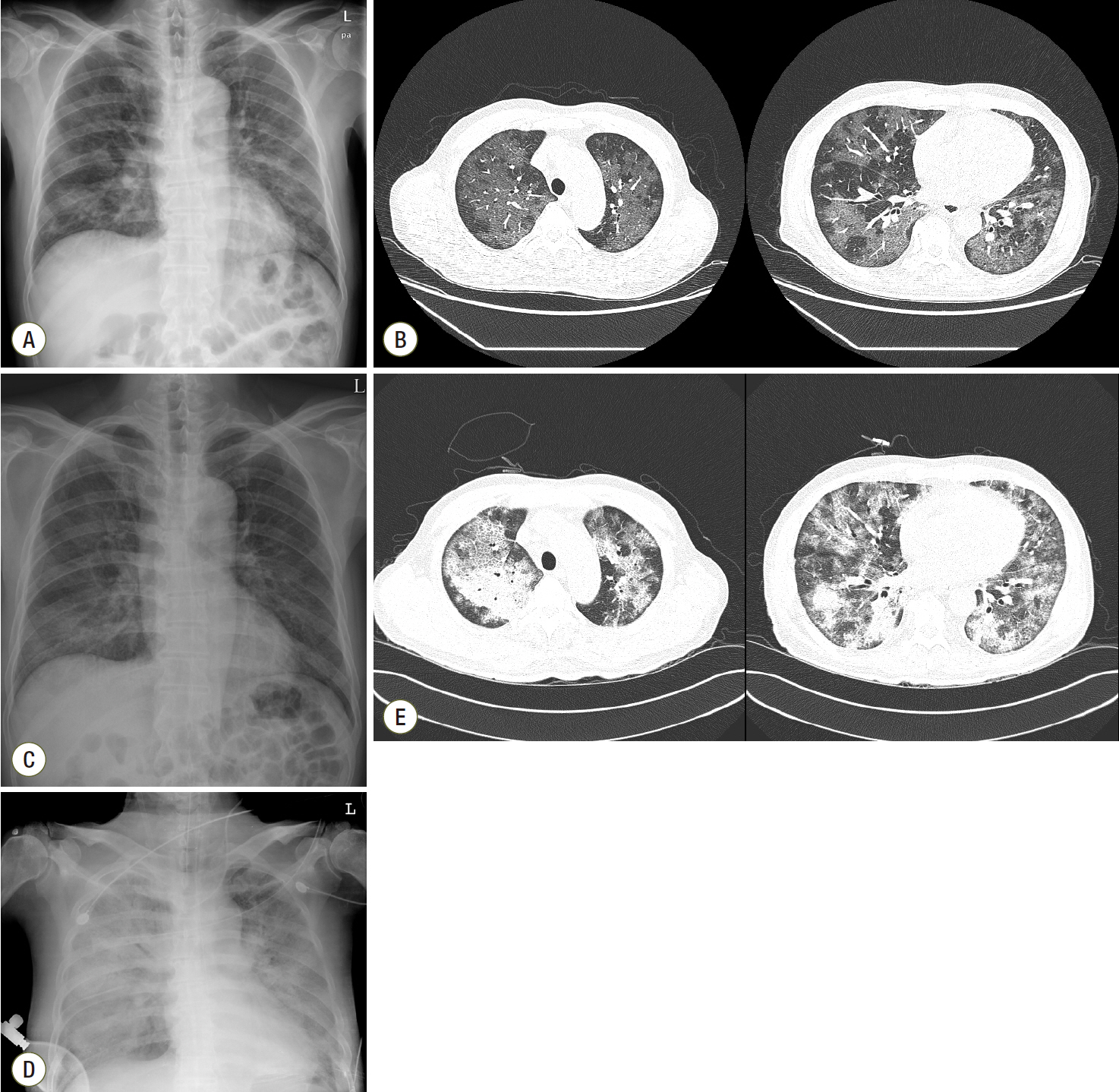
Fig. 1. Chest radiograph and computed tomography. Chest radiography and computed tomography images were obtained on hospital days 1 (A, B), 6 (C), and 19 (D, E). A and B. Chest radiographs show increased patchy opacities, and chest computed tomography reveals diffuse ground-glass opacities with a mosaic pattern in both lungs on admission. C. Chest radiography reveals mild improvement of the ground-glass density in both lungs after TMP/SMX therapy with corticosteroids on hospital day 6. D and E. Aggravated diffuse consolidation and ground-glass opacities were noted on chest radiograph and computed tomography on hospital day 19 at the time of ECMO initiation. ECMO: extracorporeal membrane oxygenation; TMP/SMX: trimethoprim/sulfamethoxazole.
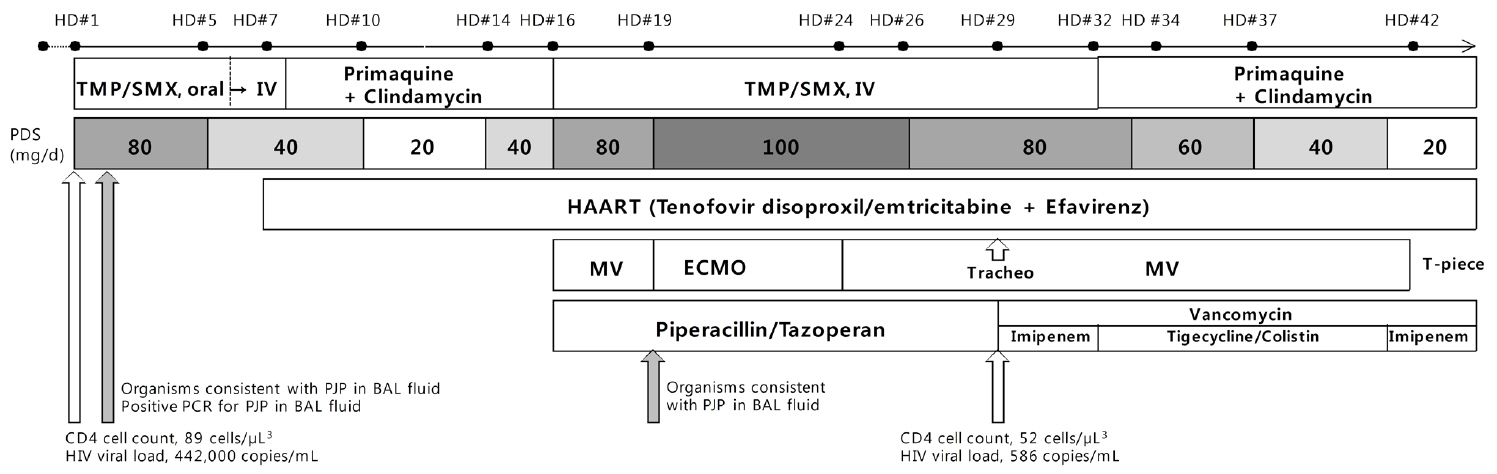
Fig. 2. Sequence of major clinical and laboratory events. HD: hospital days; TMP/SMX: trimethoprim/sulfamethoxazole; IV: intravenous; HAART: highly active antiretroviral therapy; MV: mechanical ventilation; ECMO: extracorporeal membrane oxygenation; PJP: Pnuemocystis jirovecii pneumonia; BAL: bronchoalveolar lavage; PCR: polymerase chain reaction; HIV: human immunodeficiency virus.
Reference
-
References
1. Brodie D, Bacchetta M. Extracorporeal membrane oxygenation for ARDS in adults. N Engl J Med. 2011; 365:1905–14.
Article2. Noah MA, Peek GJ, Finney SJ, Griffiths MJ, Harrison DA, Grieve R, et al. Referral to an extracorporeal membrane oxygenation center and mortality among patients with severe 2009 influenza A(H1N1). JAMA. 2011; 306:1659–68.
Article3. Peek GJ, Mugford M, Tiruvoipati R, Wilson A, Allen E, Thalanany MM, et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet. 2009; 374:1351–63.
Article4. Barbier F, Coquet I, Legriel S, Pavie J, Darmon M, Mayaux J, et al. Etiologies and outcome of acute respiratory failure in HIV-infected patients. Intensive Care Med. 2009; 35:1678–86.
Article5. Kelley CF, Checkley W, Mannino DM, Franco-Paredes C, Del Rio C, Holguin F. Trends in hospitalizations for AIDS-associated Pneumocystis jirovecii Pneumonia in the United States (1986 to 2005). Chest. 2009; 136:190–7.
Article6. Khouli H, Afrasiabi A, Shibli M, Hajal R, Barrett CR, Homel P. Outcome of critically ill human immunodeficiency virus-infected patients in the era of highly active antiretroviral therapy. J Intensive Care Med. 2005; 20:327–33.
Article7. Morris A, Wachter RM, Luce J, Turner J, Huang L. Improved survival with highly active antiretroviral therapy in HIV-infected patients with severe Pneumocystis carinii pneumonia. AIDS. 2003; 17:73–80.
Article8. Cawcutt K, Gallo De Moraes A, Lee SJ, Park JG, Schears GJ, Nemergut ME. The use of ECMO in HIV/AIDS with Pneumocystis jirovecii Pneumonia: a case report and review of the literature. ASAIO J. 2014; 60:606–8.9. De Rosa FG, Fanelli V, Corcione S, Urbino R, Bonetto C, Ricci D, et al. Extra Corporeal Membrane Oxygenation (ECMO) in three HIV-positive patients with acute respiratory distress syndrome. BMC Anesthesiol. 2014; 14:37.
Article10. Goodman JJ, Goodman LF, Sarvepalli SK, Firstenberg MS, Lustberg ME, Bazan JA. Extracorporeal Membrane Oxygenation as Adjunctive Therapy for Refractory Hypoxemic Respiratory Failure in HIV-positive Patients With Severe Pneumocystis jirovecii Pneumonia. Clin Pulm Med. 2013; 20:117–20.
Article11. Gutermann H, van Roy B, Meersseman W, Meyns B, Herijgers P. Successful extracorporeal lung assistance for overwhelming pneumonia in a patient with undiagnosed full blown aids--a controversial therapy in HIV-patients. Thorac Cardiovasc Surg. 2005; 53:252–4.12. Schmidt M, Bailey M, Sheldrake J, Hodgson C, Aubron C, Rycus PT, et al. Predicting survival after extracorporeal membrane oxygenation for severe acute respiratory failure. The Respiratory Extracorporeal Membrane Oxygenation Survival Prediction (RESP) score. Am J Respir Crit Care Med. 2014; 189:1374–82.
Article13. Barry SM, Lipman MC, Deery AR, Johnson MA, Janossy G. Immune reconstitution pneumonitis following Pneumocystis carinii pneumonia in HIV-infected subjects. HIV Med. 2002; 3:207–11.
Article14. Wislez M, Bergot E, Antoine M, Parrot A, Carette MF, Mayaud C, et al. Acute respiratory failure following HAART introduction in patients treated for Pneumocystis carinii pneumonia. Am J Respir Crit Care Med. 2001; 164:847–51.15. Zolopa A, Andersen J, Powderly W, Sanchez A, Sanne I, Suckow C, et al. Early antiretroviral therapy reduces AIDS progression/death in individuals with acute opportunistic infections: a multicenter randomized strategy trial. PLoS One. 2009; 4:e5575.
Article16. Müller M, Wandel S, Colebunders R, Attia S, Furrer H, Egger M, et al. Immune reconstitution inflammatory syndrome in patients starting antiretroviral therapy for HIV infection: a systematic review and meta-analysis. Lancet Infect Dis. 2010; 10:251–61.
Article17. Huang L, Cattamanchi A, Davis JL, den Boon S, Kovacs J, Meshnick S, et al. HIV-associated Pneumocystis pneumonia. Proc Am Thorac Soc. 2011; 8:294–300.
Article18. National Institutes of Health; AIDSinfo. Guidelines for prevention and treatment of opportunistic infections in HIV-infected adults and adolescents. 2016. May. [2016 May]. Available from https://aidsinfo.nih.gov/guidelines/html/4/adult-and-adolescent-oi-prevention-andtreatment-guidelines/0.19. Helweg-Larsen J, Benfield T, Atzori C, Miller RF. Clinical efficacy of first- and second-line treatments for HIV-associated Pneumocystis jirovecii pneumonia: a tri-centre cohort study. J Antimicrob Chemother. 2009; 64:1282–90.
Article20. Paden ML, Conrad SA, Rycus PT, Thiagarajan RR, ELSO Registry. Extracorporeal Life Support Organization Registry Report 2012. ASAIO J. 2013; 59:202–10.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Unmasking Granulomatous Pneumocystis jirovecii Pneumonia with Nodular Opacity in an HIV-Infected Patient after Initiation of Antiretroviral Therapy
- Extracorporeal Membrane Oxygenation Therapy for Aspiration Pneumonia in a Patient following Left Pneumonectomy for Lung Cancer
- Pneumocystis jirovecii Pneumonia Accompanied with Fat Embolism: A Case Report
- Successful use of extracorporeal membrane oxygenation for sudden aggravation of acute respiratory distress syndrome: A case report
- Successful Treatment in Fatal Adenovirus Pneumonia with the Use of Extracorporeal Membrane Oxygenation
