J Korean Med Assoc.
2010 Nov;53(11):1006-1014.
Treatment of varicose vein
- Affiliations
-
- 1Department of Thoracic and Cardiovascular Surgery, Chung-Ang University College of Medicine, Seoul, Korea. cadywk@cau.ac.kr
Abstract
- High venous pressure in leg from walking in erect position can lead the development of defective valves and reflux, and superficial veins may become elongated and tortuous. Women are more prone to varicose vein due to hormonal influences and pregnancy. Besides long standing occupation and female gender, there are other risk factors including age, family history, obesity, and prior deep vein thrombosis. Recently developed health related quality of life has contributed to concern more about varicose vein and develop the treatment modalities of varicose vein. Because of the chronicity of the development of varicose vein, most patients are usually accustomed to high venous pressure of their leg and feel minor or no discomfort. Among the reasons to seek for the treatment of varicose vein, cosmetic purpose is the most common. Most patients prefer non-surgical treatment including sclerotheraphy to surgical intervention. High ligation and stripping of varicose vein has remained as the standard treatment of varicose vein with excellent long term results. Minimal invasive non-surgical treatments including radiofrequency ablation and endovenous laser treatment have shown less scars and earlier mobility. Newer treatment modalities have to prove comparable long term results, not merely better cosmetic and short term results. We reviewed about the development of varicose vein and the treatment modalities including preventive measures. Correct comprehension of the patient and proper application of the treatment modality are essential for the good result without recurrence after the treatment of varicose vein.
MeSH Terms
Figure
-
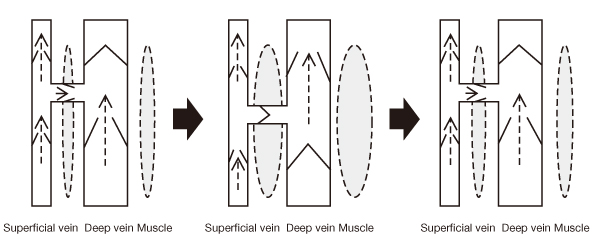
Figure 1 Schematic drawing of muscle pump. The deep vein is surrounded by the calf muscle. During muscle relaxation, the deep vein is filled with the blood from distal part and the superficial vein through the perforating vein. During contraction, muscle eject the blood from the deep vein to the heart and the valves in the perforating vein are closed to block the flow from the deep vein to the superficial vein.
Reference
-
1. Naoum JJ, Hunter GC. Pathogenesis of varicose veins and implications for clinical management. Vascular. 2007. 15:242–249.
Article2. Goldman MP, Fronek A. Anatomy and pathophysiology of varicose veins. J Dermatol Surg Oncol. 1989. 15:138–145.
Article3. Suh BY. Varicose veins in the legs. J Korean Soc Phlebol. 2002. 1:3–8.4. Lim CS, Davies AH. Pathogenesis of primary varicose veins. Br J Surg. 2009. 96:1231–1242.
Article5. Caggiati A, Rosi C, Heyn R, Franceschini M, Acconcia MC. Age-related variations of varicose veins anatomy. J Vasc Surg. 2006. 44:1291–1295.
Article6. Dodd H. The varicose tributaries of the popliteal vein. Br J Surg. 1965. 52:350–354.7. Perkins JM. Standard varicose vein surgery. Phlebology. 2009. 24:Suppl 1. 34–41.
Article8. Teruya TH, Ballard JL. New approaches for the treatment of varicose veins. Surg Clin North Am. 2004. 84:1397–1417.
Article9. Jones RH, Carek PJ. Management of varicose veins. Am Fam Physician. 2008. 78:1289–1294.10. Hirsch SA, Dillavou E. Options in the management of varicose veins, 2008. J Cardiovasc Surg (Torino). 2008. 49:19–26.11. Kouri B. Current evaluation and treatment of lower extremity varicose veins. Am J Med. 2009. 122:513–515.
Article12. Leopardi D, Hoggan BL, Fitridge RA, Woodruff PW, Maddern GJ. Systematic review of treatments for varicose veins. Ann Vasc Surg. 2009. 23:264–276.
Article13. van den Bremer J, Moll FL. Historical overview of varicose vein surgery. Ann Vasc Surg. 2010. 24:426–432.
Article14. Sam RC, Silverman SH, Bradbury AW. Nerve injuries and varicose vein surgery. Eur J Vasc Endovasc Surg. 2004. 27:113–120.
Article15. Beale RJ, Gough MJ. Treatment options for primary varicose veins: a review. Eur J Vasc Endovasc Surg. 2005. 30:83–95.16. Sadick NS. Advances in the treatment of varicose veins: ambulatory phlebectomy, foam sclerotherapy, endovascular laser, and radiofrequency closure. Adv Dermatol. 2006. 22:139–156.
Article17. Tremblay J, Lewis EW, Allen PT. Selecting a treatment for primary varicose veins. Can Med Assoc J. 1985. 133:20–25.18. de Groot WP. Treatment of varicose veins: modern concepts and methods. J Dermatol Surg Oncol. 1989. 15:191–198.
Article19. Jia X, Mowatt G, Burr JM, Cassar K, Cook J, Fraser C. Systematic review of foam sclerotherapy for varicose veins. Br J Surg. 2007. 94:925–936.
Article20. Nootheti PK, Cadag KM, Goldman MP. Review of intravascular approaches to the treatment of varicose veins. Dermatol Surg. 2007. 33:1149–1157.
Article21. Hoggan BL, Cameron AL, Maddern GJ. Systematic review of endovenous laser therapy versus surgery for the treatment of saphenous varicose veins. Ann Vasc Surg. 2009. 23:277–287.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Recent Overview of Varicose Vein in the Legs
- Successful use of VenaSeal system for the treatment of large great saphenous vein of 2.84-cm diameter
- Overexpression of Estrogen Receptor in Female Patients with Varicose Vein of Lower Extremities
- Varicose Vein Caused by Giant Hydronephrosis Associated with Horseshoe Kidney
- Pretibial Varicose Vein from Intraosseous Perforating Vein Incompetence
