An Extramedullary Femoral Alignment System in Total Knee Arthroplasty Using the Inter-Femoral Head Center Distance
- Affiliations
-
- 1Department of Orthopedic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. medisoon@naver.com
Abstract
- PURPOSE
Total knee arthroplasty using the extramedullary technique for alignment has some difficulty for detecting the center of the femoral head intra-operatively. In this study we tried to evaluate the usefulness and accuracy of a newly developed Mechanical Axis Marker that synchronizes the center of the knee joint and femoral head with the mechanical axis for the distal femoral cutting and femoral prosthesis alignment. MATERIALS AND
METHODS
Between October 2008 and January 2009, 255 knees in 156 patients underwent total knee arthroplasty. We measured the distance between each centers of the femoral head using the PACS system and we applied the distance to the newly developed Mechanical Axis Marker. Subsequently, we applied the new marker to patients to align the centers of knee, the femoral head and the marker in line with the mechanical axis intra-operatively. The accuracy of the marker was validated with C-arm fluoroscopy pre-operatively in 20 patients. Post-operatively we measured and analyzed the frontal femoral component angle to evaluate the coronal alignment of the femoral implant. The accuracy was rated as excellent when the alignment was <3degrees, as good when the alignment was 3-5degrees, and as poor when the alignment was >5degrees.
RESULTS
The pre-operative validation study with the C-arm fluoroscopy showed that the distance between the femoral head center and the metal peg of the marker was within 5 mm in 95% of the patients, which implied acceptable accuracy. The average frontal femoral component angle against the mechanical axis was 89.0degrees+/-1.1 (range 86degrees-96.6degrees). The proportion of excellent, good, and poor alignments was 90.6% (231 cases), 8.6% (22 cases), and 0.8% (2 cases), respectively. The intraclass correlation coefficient between the two observers for the frontal femoral component angle was 0.972 which showed high concordance.
CONCLUSION
Our results indicate that the extramedullary technique assisted by our new Mechanical Axis Marker can easily identify the center of femoral head and improve the accuracy of frontal femoral component alignment with the proper mechanical axis.
Keyword
MeSH Terms
Figure
-
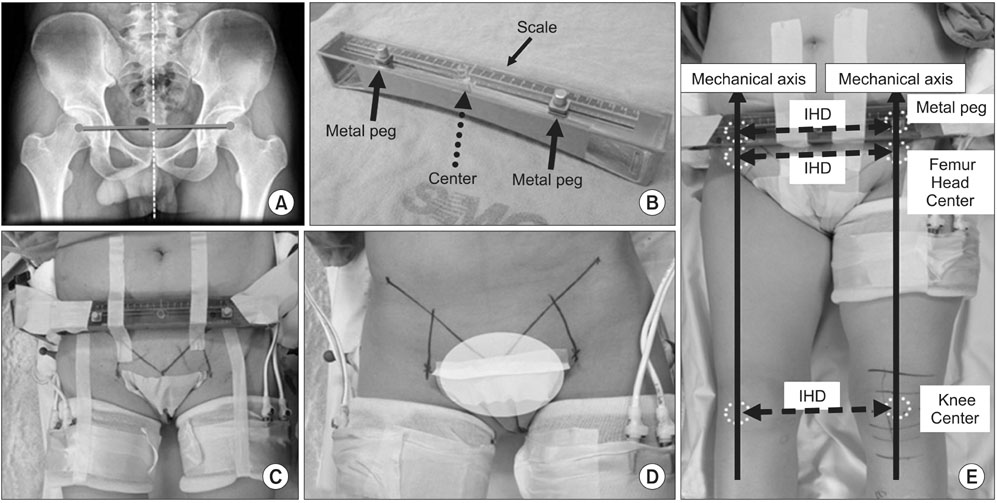
Figure 1 Mechanical axis is extramedullarily aligned using Mechanical Axis Marker. (A) X-ray shows the inter-femoral head center distance. (B) The Mechanical Axis Marker: the plastic rod and metal pegs were used to simulate inter-femoral head center distance. Black solid arrows indicate metal pegs. (C) The Mechanical Axis Marker was equipped to patients. (D) The lines indicating inguinal ligaments and the flow of femoral artery are drawn pre-operatively. (E) The mechanical axis which is the line between Metal peg (estimated femoral head center) and knee center is easily recognized during operation using this device. IHD, inter-femoral head distance.
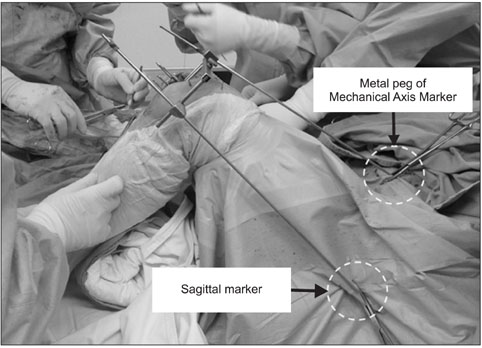
Figure 2 Extramedullary alignment method using Mechanical Axis Marker, sagittal marker and two guide rods during operation.
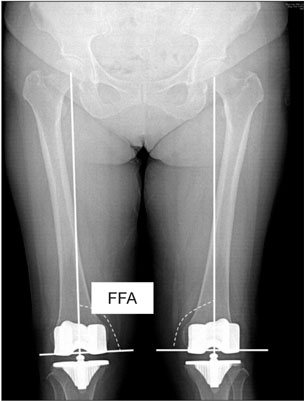
Figure 3 A radiograph showing the mechanical axis in the coronal plane. The alignment of the coronal femoral components was measured by the intersection of a line drawn across the base of each component and the mechanical axis. FFA, frontal femoral angle.
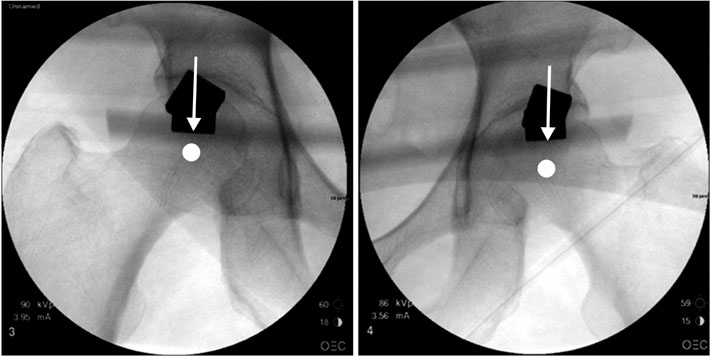
Figure 4 Accuracy of Mechanical Axis Marker was validated using C-arm. Representative pictures are shown among 20 patients.
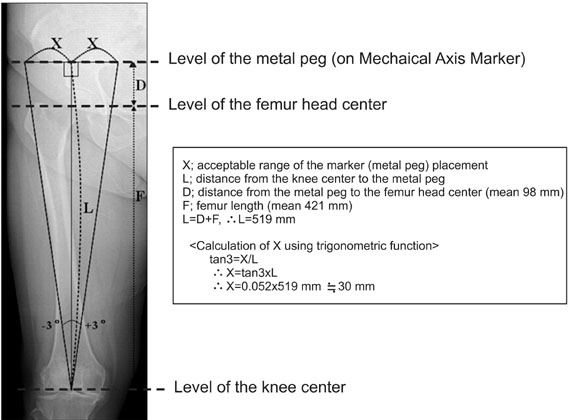
Figure 5 Acceptable range of error in Mechanical Axis Marker placement.
Reference
-
1. Bai B, Baez J, Testa N, Kummer FJ. Effect of posterior cut angle on tibial component loading. J Arthroplasty. 2000. 15:916–920.
Article2. Mihalko WM, Krackow KA. Posterior cruciate ligament effects on the flexion space in total knee arthroplasty. Clin Orthop Relat Res. 1999. 360:243–250.
Article3. Matsuda S, Miura H, Nagamine R, et al. Posterior tibial slope in the normal and varus knee. Am J Knee Surg. 1999. 12:165–168.4. Laskin RS. Total knee arthroplasty using an uncemented, polyethylene tibial implant. A seven-year follow-up study. Clin Orthop Relat Res. 1993. 288:270–276.
Article5. Andriacchi TP. Biomechanics and gait analysis in total knee replacement. Orthop Rev. 1988. 17:470–473.6. Matsuda Y, Ishii Y, Ichimura K. Identifying the center of the femoral head using ultrasonography to assess the higher accuracy of femoral extramedullary guides in TKA. J Orthop Sci. 2004. 9:6–9.
Article7. Ritter MA, Herbst SA, Keating EM, Faris PM, Meding JB. Long-term survival analysis of a posterior cruciate-retaining total condylar total knee arthroplasty. Clin Orthop Relat Res. 1994. 309:136–145.8. Hvid I, Nielsen S. Total condylar knee arthroplasty. Prosthetic component positioning and radiolucent lines. Acta Orthop Scand. 1984. 55:160–165.
Article9. Insall JN. Surgery of the knee. 1984. New York: Churchill Livingstone;587–696.10. Jeffery RS, Morris RW, Denham RA. Coronal alignment after total knee replacement. J Bone Joint Surg Br. 1991. 73:709–714.
Article11. Rand JA, Coventry MB. Ten-year evaluation of geometric total knee arthroplasty. Clin Orthop Relat Res. 1988. 232:168–173.
Article12. Bargren JH, Blaha JD, Freeman MA. Alignment in total knee arthroplasty. Correlated biomechanical and clinical observations. Clin Orthop Relat Res. 1983. 173:178–183.13. Lotke PA, Ecker ML. Influence of positioning of prosthesis in total knee replacement. J Bone Joint Surg Am. 1977. 59:77–79.
Article14. Baldini A, Adravanti P. Less invasive TKA: extramedullary femoral reference without navigation. Clin Orthop Relat Res. 2008. 466:2694–2700.15. Yoo JH, Han DY, Han CD, et al. Intramedullary and extramedullary combined alignment system for tibial component placement in total knee arthroplasty. J Korean Knee Soc. 2004. 16:118–124.16. Cates HE, Ritter MA, Keating EM, Faris PM. Intramedullary versus extramedullary femoral alignment systems in total knee replacement. Clin Orthop Relat Res. 1993. 286:32–39.
Article17. Dennis DA, Channer M, Susman MH, Stringer EA. Intramedullary versus extramedullary tibial alignment systems in total knee arthroplasty. J Arthroplasty. 1993. 8:43–47.
Article18. Brys DA, Lombardi AV Jr, Mallory TH, Vaughn BK. A comparison of intramedullary and extramedullary alignment systems for tibial component placement in total knee arthroplasty. Clin Orthop Relat Res. 1991. 263:175–179.
Article19. Engh GA, Petersen TL. Comparative experience with intramedullary and extramedullary alignment in total knee arthroplasty. J Arthroplasty. 1990. 5:1–8.
Article20. Tillett ED, Engh GA, Petersen T. A comparative study of extramedullary and intramedullary alignment systems in total knee arthroplasty. Clin Orthop Relat Res. 1988. 230:176–181.
Article21. Kandel L, Vasili C, Kirsh G. Extramedullary femoral alignment instrumentation reduces blood loss after uncemented total knee arthroplasty. J Knee Surg. 2006. 19:256–258.
Article22. Kumar N, Saleh J, Gardiner E, Devadoss VG, Howell FR. Plugging the intramedullary canal of the femur in total knee arthroplasty: reduction in postoperative blood loss. J Arthroplasty. 2000. 15:947–949.23. Markel DC, Femino JE, Farkas P, Markel SF. Analysis of lower extremity embolic material after total knee arthroplasty in a canine model. J Arthroplasty. 1999. 14:227–232.
Article24. Sawant MR, Murty A, Ireland J. A clinical method for locating the femoral head centre during total knee arthroplasty. Knee. 2004. 11:209–212.
Article25. Seo JG, Kim BK, Moon YW, et al. Bony landmarks for determining the mechanical axis of the femur in the sagittal plane during total knee arthroplasty. Clin Orthop Surg. 2009. 1:128–131.
Article26. Teter KE, Bregman D, Colwell CW Jr. The efficacy of intramedullary femoral alignment in total knee replacement. Clin Orthop Relat Res. 1995. 321:117–121.
Article27. Shin YH, Kim MH, Ko JS, Park JA. The safety of simultaneous bilateral versus unilateral total knee arthroplasty: the experience in a Korean hospital. Singapore Med J. 2010. 51:44–49.28. Novak EJ, Silverstein MD, Bozic KJ. The cost-effectiveness of computer-assisted navigation in total knee arthroplasty. J Bone Joint Surg Am. 2007. 89:2389–2397.
Article29. Stulberg SD, Yaffe MA, Koo SS. Computer-assisted surgery versus manual total knee arthroplasty: a case-controlled study. J Bone Joint Surg Am. 2006. 88:Suppl 4. 47–54.
Article30. Seo JG, Moon YW, Kim YS. A comparison of extramedullary and intramedullary femoral component alignment guide systems in TKA. J Korean Knee Soc. 2006. 18:47–54.31. Jenny JY, Boeri C, Ballonzoli L. Coronal alignment of the lower limb. Acta Orthop. 2005. 76:403–407.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Accuracy of Inter Femoral Head Center Distance Measurement and Evaluation for Coronal Alignment of Femoral Component during Total Knee Arthroplasty
- A Comparison of Accuracy between the Sonography-guided Extramedullary and Intramedullary Alignment Systems for the Femoral Component in Total Knee Arthroplasty
- A Comparison of Extramedullary and Intramedullary Femoral Component Alignment Guide Systems in TKA
- Easy Identification of Mechanical Axis during Total Knee Arthroplasty
- Efficacy of Extramedullary Femoral Component Alignment Guide System for Blood Saving after Total Knee Arthroplasty
