Ann Rehabil Med.
2016 Jun;40(3):540-544. 10.5535/arm.2016.40.3.540.
Bilateral Anterior Opercular Syndrome With Partial Kluver-Bucy Syndrome in a Stroke Patient: A Case Report
- Affiliations
-
- 1Department of Rehabilitation Medicine, Hallym University Chuncheon Sacred Heart Hospital, Hallym University College of Medicine, Chuncheon, Korea. jylimmd@eulji.ac.kr
- 2Department of Rehabilitation Medicine, Eulji University Hospital, Daejeon, Korea.
- KMID: 2327618
- DOI: http://doi.org/10.5535/arm.2016.40.3.540
Abstract
- Bilateral anterior opercular syndrome and partial Kluver-Bucy syndrome are associated with bilateral middle cerebral artery lesions. The combination of these two syndromes has only been reported in a child with limbic encephalitis. In this case, a 44-year-old woman with bilateral middle cerebral artery infarction, which occurred 2 years prior, could walk independently. However, she showed automatic-voluntary dissociation and anarthria with preserved writing skills. She also presented hypersexuality, hypermetamorphosis, and memory disturbances. Here, we report a case of an adult stroke patient who suffered from bilateral anterior opercular syndrome accompanied by partial Kluver-Bucy syndrome.
MeSH Terms
Figure
-
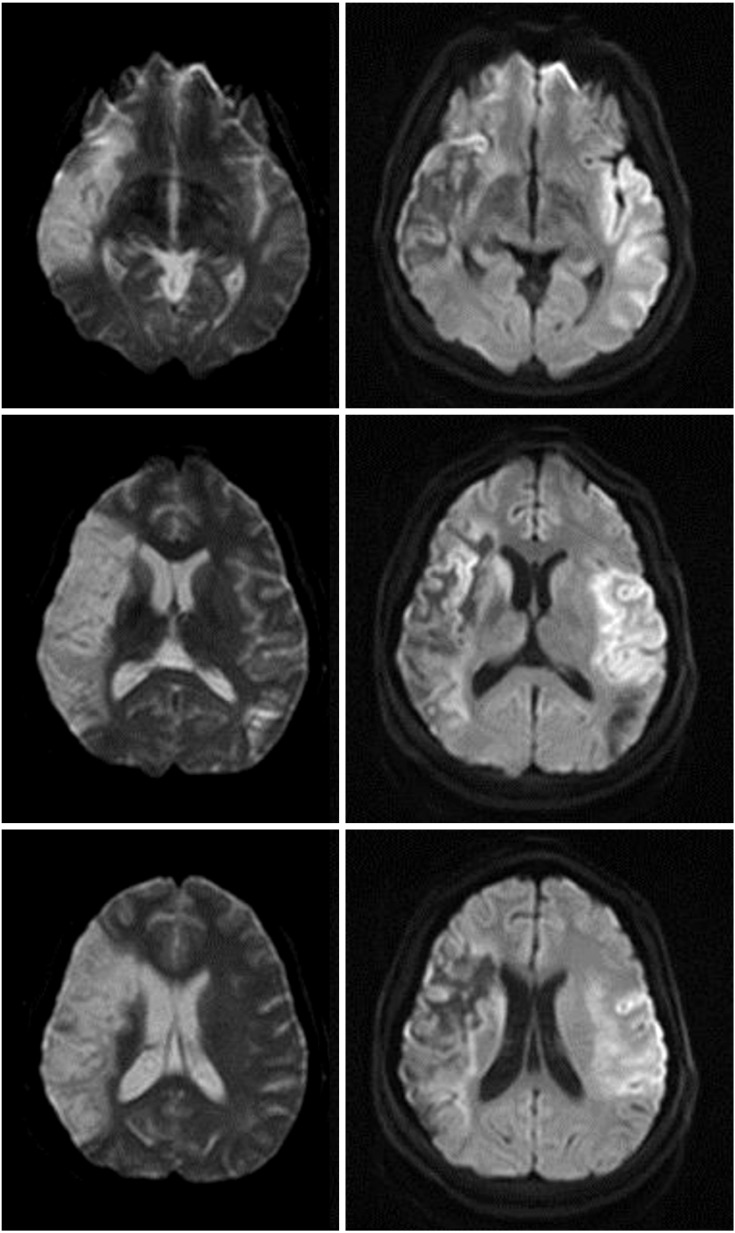
Fig. 1 Brain diffusion magnetic resonance imaging with b=0 (left) and b=1,000 (right) showed subacute right middle cerebral artery infarction (left) and acute left middle cerebral artery infarction (right), including the bilateral anterior operculum.
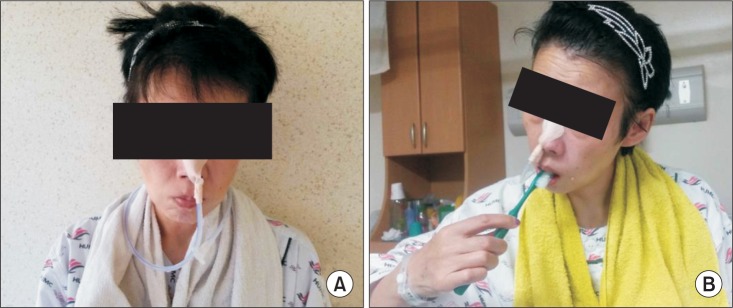
Fig. 2 On the administration day, she tried to open her mouth and she could not (A). After 4 weeks of training, the patient could brush her teeth by herself (B).
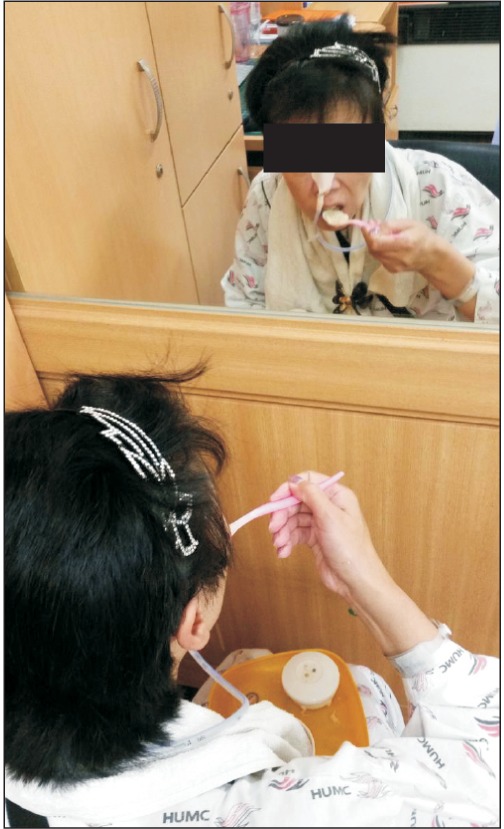
Fig. 3 The patient was trained in opening her mouth and semisolid swallowing in front of the mirror.
Reference
-
1. Lekhjung T, Raju P. Opercular syndrome: case reports and review of literature. Neurol Asia. 2010; 15:145–152.2. Weller M. Anterior opercular cortex lesions cause dissociated lower cranial nerve palsies and anarthria but no aphasia: Foix-Chavany-Marie syndrome and "automatic voluntary dissociation" revisited. J Neurol. 1993; 240:199–208. PMID: 7684439.
Article3. Chou CL, Lin YJ, Sheu YL, Lin CJ, Hseuh IH. Persistent Kluver-Bucy syndrome after bilateral temporal lobe infarction. Acta Neurol Taiwan. 2008; 17:199–202. PMID: 18975528.4. Bhat PS, Pardal PK, Das RC. Partial Kluver-Bucy syndrome as a delayed manifestation of head injury. Ind Psychiatry J. 2009; 18:117–118. PMID: 21180489.
Article5. Kar SK, Jaiswal A, Panda AK. A case report of partial Kluver-Bucy syndrome with anterior opercular syndrome in childhood: a sequel of limbic encephalitis. J Indian Assoc Child Adolesc Ment Health. 2013; 9:80–88.6. Nowak DA, Griebl G, Dabitz R, Ochs G. Bilateral anterior opercular (Foix-Chavany-Marie) syndrome. J Clin Neurosci. 2010; 17:1441–1442. PMID: 20655752.
Article7. Mao CC, Coull BM, Golper LA, Rau MT. Anterior operculum syndrome. Neurology. 1989; 39:1169–1172. PMID: 2771066.
Article8. Milanlioglu A, Aydin MN, Gokgul A, Hamamci M, Erkuzu MA, Tombul T. Ischemic bilateral opercular syndrome. Case Rep Med. 2013; 2013:513572. PMID: 23476665.
Article9. Kim DE, Lee YS, Park SH, Park KI, Cho JY, Kim SS, et al. A case of bilateral anterior opercular syndrome: Foix-Chavany-Marie syndrome. J Korean Neurol Assoc. 2000; 18:450–453.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Kluver-Bucy Syndrome Following Bilateral Posterior Cerebral Artery Infarction
- Relapsing Herpes Simplex Encephalitis Resulting in Kluver-Bucy Syndrome
- Transient Hyperorality during Automotor Seizure in a Patient with Right Temporal Lobe Epilepsy. Epileptic Kluver-Bucy Syndrome?
- A Case of Bilateral Anterior Opercular Syndrome: Foix-Chavany-Marie Syndrome
- A case of Pick's disease presenting with progressive nonfluent speech
