Imaging Features of Infratentorial Desmoplastic Infantile and Non-Infantile Tumors
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiological Science, Severance Children's Hospital, Yonsei University College of Medicine, Seoul, Korea. mjl1213@yuhs.ac
- 2Department of Radiology, Ajou University School of Medicine, Ajou University Medical Center, Suwon, Korea.
- 3Department of Pathology, Yonsei University College of Medicine, Severance Hospital, Seoul, Korea.
- KMID: 2327367
- DOI: http://doi.org/10.3348/jksr.2016.75.1.49
Abstract
- PURPOSE
To describe imaging features of infratentorial desmoplastic infantile or non-infantile tumors (DIT/DNIT).
MATERIALS AND METHODS
Four cases with infratentorial DIT/DNIT from our hospital and 5 cases from literature review were analyzed. Clinical data and MR imaging features were evaluated including location, size, shape, margin, composition, dural attachment, perilesional edema, and metastasis or multiplicity.
RESULTS
The mean age was 9.2 years (range, 1-18 years). Most of the patients presented with headache or vomiting (4/9, 44.4%) and had no underlying disease (8/9, 88.9%). The major pathologic subtype was astrocytoma (6/9, 66.7%). On MR, majority of the tumors involved cerebellum and/or spinal cord (8/9, 88.9%) and the mean size of the tumors was 4.2 cm (range, 3.2-5 cm). The tumors were mainly solid (4/9, 44.4%) or mixed (4/9, 44.4%) in composition with lobulated shape (7/9, 77.8%) and well-defined margin (7/9, 77.8%). Two cases (2/7, 28.6%) showed dural attachment and all the cases had no or minimal perilesional edema (100%). Metastasis or multiplicity was frequently seen in 44.4% (4/9).
CONCLUSION
Infratentorial DIT/DNIT occurred in relatively older children and the major tumor type was astrocytoma. They also had atypical imaging features showing mainly solid or mixed in composition with frequent metastasis or multiplicity.
MeSH Terms
Figure
-
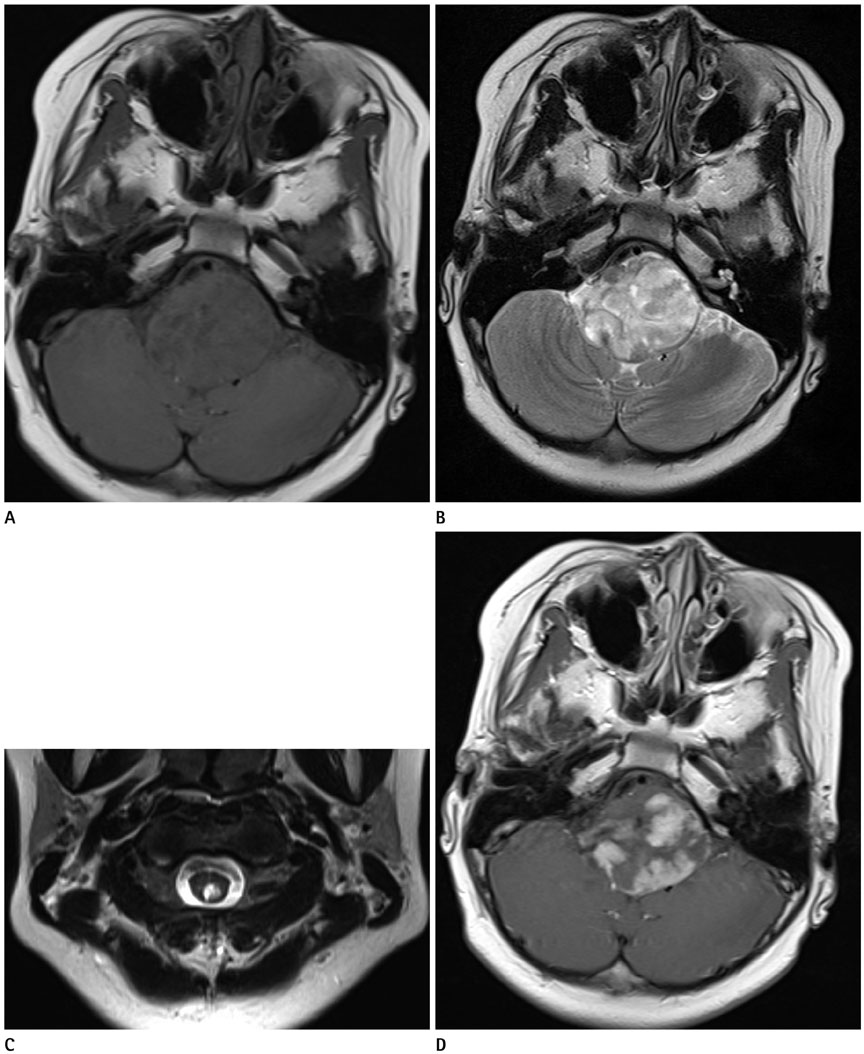
Fig. 1 Case 1. A six-year-old boy with desmoplastic non-infantile astrocytoma. A mass involving the medulla oblongata and upper cervical spinal cord demonstrates mainly solid composition with isointense to parenchyma on T1-weighted image (A), high signal intensity on T2-weighted image (B, C), and heterogeneous enhancement in the solid portion on contrast enhancement study (D).
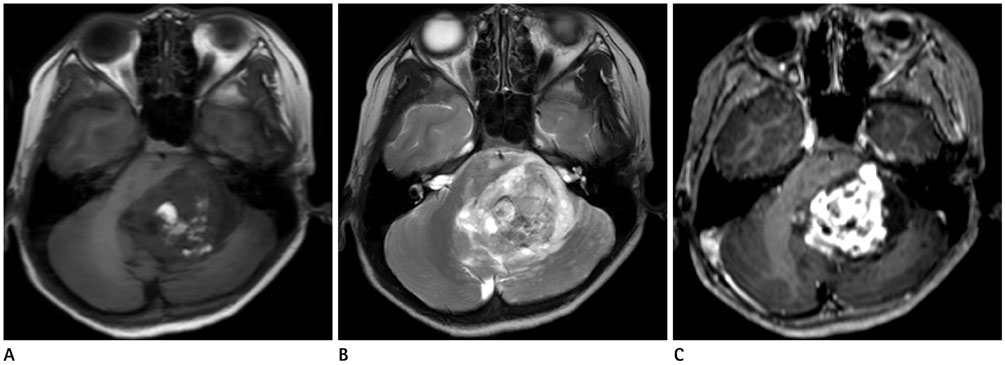
Fig. 2 Case 2. A nine-year-old boy with desmoplastic non-infantile astrocytoma. A mass involving the cerebellum and midbrain shows high signal intensity areas of fat on T1-weighted image (A), solid portion with multiple small cystic lesions on T2-weighted image (B), and heterogeneous enhancement in the solid portion on contrast enhancement study (C).
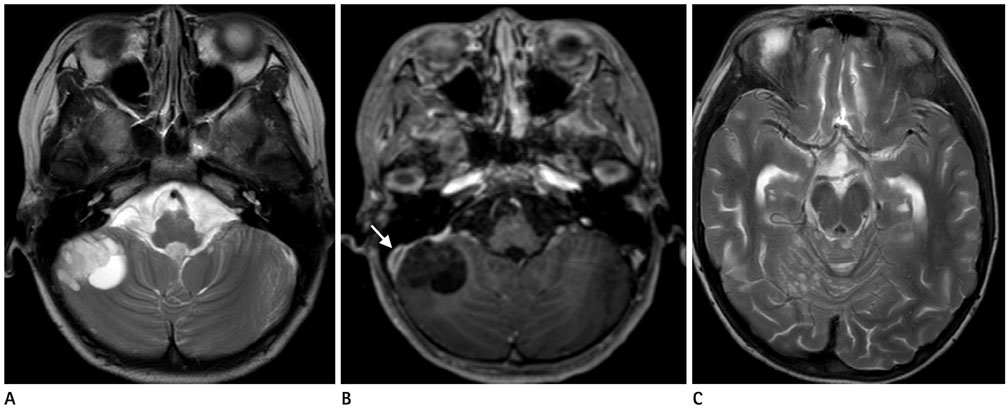
Fig. 3 Case 3. A nine-year-old girl with desmoplastic non-infantile astrocytoma. A mass in the right cerebellum demonstrates entirely cystic on T2-weighted image (A), internal septation and dural attachment (arrow) on contrast enhancement T1-weighted image (B), and multiple small cystic lesions in the cerebellum (C).
Reference
-
1. VandenBerg SR, May EE, Rubinstein LJ, Herman MM, Perentes E, Vinores SA, et al. Desmoplastic supratentorial neuroepithelial tumors of infancy with divergent differentiation potential ("desmoplastic infantile gangliogliomas"). Report on 11 cases of a distinctive embryonal tumor with favorable prognosis. J Neurosurg. 1987; 66:58–71.2. Rout P, Santosh V, Mahadevan A, Kolluri VR, Yasha TC, Shankar SK. Desmoplastic infantile ganglioglioma--clinicopathological and immunohistochemical study of four cases. Childs Nerv Syst. 2002; 18:463–467.3. Ng TH, Fung CF, Ma LT. The pathological spectrum of desmoplastic infantile gangliogliomas. Histopathology. 1990; 16:235–241.4. Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC, Jouvet A, et al. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol. 2007; 114:97–109.5. Tenreiro-Picon OR, Kamath SV, Knorr JR, Ragland RL, Smith TW, Lau KY. Desmoplastic infantile ganglioglioma: CT and MRI features. Pediatr Radiol. 1995; 25:540–543.6. Trehan G, Bruge H, Vinchon M, Khalil C, Ruchoux MM, Dhellemmes P, et al. MR imaging in the diagnosis of desmoplastic infantile tumor: retrospective study of six cases. AJNR Am J Neuroradiol. 2004; 25:1028–1033.7. De Munnynck K, Van Gool S, Van Calenbergh F, Demaerel P, Uyttebroeck A, Buyse G, et al. Desmoplastic infantile ganglioglioma: a potentially malignant tumor? Am J Surg Pathol. 2002; 26:1515–1522.8. Milanaccio C, Nozza P, Ravegnani M, Rossi A, Raso A, Gambini C. Cervico-medullary desmoplastic infantile ganglioglioma: an unusual case with diffuse leptomeningeal dissemination at diagnosis. Pediatr Blood Cancer. 2005; 45:986–990.9. Darwish B, Arbuckle S, Kellie S, Besser M, Chaseling R. Desmoplastic infantile ganglioglioma/astrocytoma with cerebrospinal metastasis. J Clin Neurosci. 2007; 14:498–501.10. Lönnrot K, Terho M, Kähärä V, Haapasalo H, Helén P. Desmoplastic infantile ganglioglioma: novel aspects in clinical presentation and genetics. Surg Neurol. 2007; 68:304–308. discussion 308.11. Santhosh K, Kesavadas C, Radhakrishnan VV, Abraham M, Gupta AK. Multifocal desmoplastic noninfantile astrocytoma. J Neuroradiol. 2008; 35:286–291.12. Rasalkar DD, Paunipagar BK, Ng A. Primary spinal cord desmoplastic astrocytoma in an adolescent: a rare tumour at rare site and rare age. Hong Kong Med J. 2012; 18:253–255.13. Gundamaneni SK, Ganesh CV, Mahadevan A, Madhugiri VS, Sasidharan GM, Kumar VR. Non-infantile desmoplastic cerebellar ganglioglioma in a patient with multiple congenital anomalies: a rare association. Pediatr Neurosurg. 2013; 49:105–109.14. Taranath A, Lam A, Wong CK. Desmoplastic infantile ganglioglioma: a questionably benign tumour. Australas Radiol. 2005; 49:433–437.15. Setty SN, Miller DC, Camras L, Charbel F, Schmidt ML. Desmoplastic infantile astrocytoma with metastases at presentation. Mod Pathol. 1997; 10:945–951.16. Karabagli P, Karabagli H, Kose D, Kocak N, Etus V, Koksal Y. Desmoplastic non-infantile astrocytic tumor with BRAF V600E mutation. Brain Tumor Pathol. 2014; 31:282–288.17. Taguchi Y, Sakurai T, Takamori I, Sekino H, Tadokoro M. Desmoplastic infantile ganglioglioma with extraparenchymatous cyst--case report. Neurol Med Chir (Tokyo). 1993; 33:177–180.18. Gelabert-Gonzalez M, Serramito-García R, Arcos-Algaba A. Desmoplastic infantile and non-infantile ganglioglioma. Review of the literature. Neurosurg Rev. 2010; 34:151–158.19. Tortori-Donati P, Rossi A, Biancheri R, Garrè ML, Cama A. Brain tumors. In : Tortori-Donati P, Rossi A, Biancheri R, Garrè ML, Cama A, editors. Pediatric neuroradiology. Berlin: Springer;2005. p. 329–436.20. Houten JK, Weiner HL. Pediatric intramedullary spinal cord tumors: special considerations. J Neurooncol. 2000; 47:225–230.21. Nemoto Y, Inoue Y, Tashiro T, Mochizuki K, Oda J, Kogame S, et al. Intramedullary spinal cord tumors: significance of associated hemorrhage at MR imaging. Radiology. 1992; 182:793–796.
