J Korean Soc Radiol.
2013 May;68(5):397-405.
Relationship between Conventional Cardiovascular Disease Risk Assessment and Coronary Artery Calcification in Group Exposed to Inorganic Dusts
- Affiliations
-
- 1Occupational Lung Diseases Institute, KCOMWEL, Ansan, Korea. atomlwj@gmail.com
Abstract
- PURPOSE
The purpose of this study is to determine the relationship between the coronary artery calcification (CAC) and the conventional cardiovascular disease risk assessment (CCDRA).
MATERIALS AND METHODS
This study included 101 subjects who were exposed to inorganic dusts and underwent CAC scoring by multidetector CT (MDCT), laboratory tests, and a standardized questionnaire for CCDRA, after being approved from the Institutional Review Board and providing informed consent. All subjects were divided as either non-calcified group (< 1, 55.4%) or calcified group (> or = 1, 44.6%) from total CAC, and evaluated by CCDRA, such as Framingham risk score (FRS) and National Cholesterol Education Program (NCEP). Receiver operating characteristic (ROC) area of FRS was generated for predicting CAC risk using SPSS program (ver. 19.0, Chicago, IL, USA).
RESULTS
Total CAC was significantly correlated with FRS (r = 0.283, p = 0.004). Crude odds ratio for CAC risk was 3.64 [95% confidence interval (CI) 1.39-9.52] in FRS > or = 20%, and 2.87 (95% CI 1.24-6.65) in the high risk group of NCEP. Subjects with pneumoconiosis showed higher values of CAC (p = 0.541) and FRS (p = 0.035) scores compared with subjects without pneumoconiosis. ROC area of FRS was 0.69 (95% CI 0.59-0.79) with a cutoff point of 13.5%.
CONCLUSION
CAC measured MDCT is significantly correlated with FRS than other CCDRA.
MeSH Terms
Figure
-
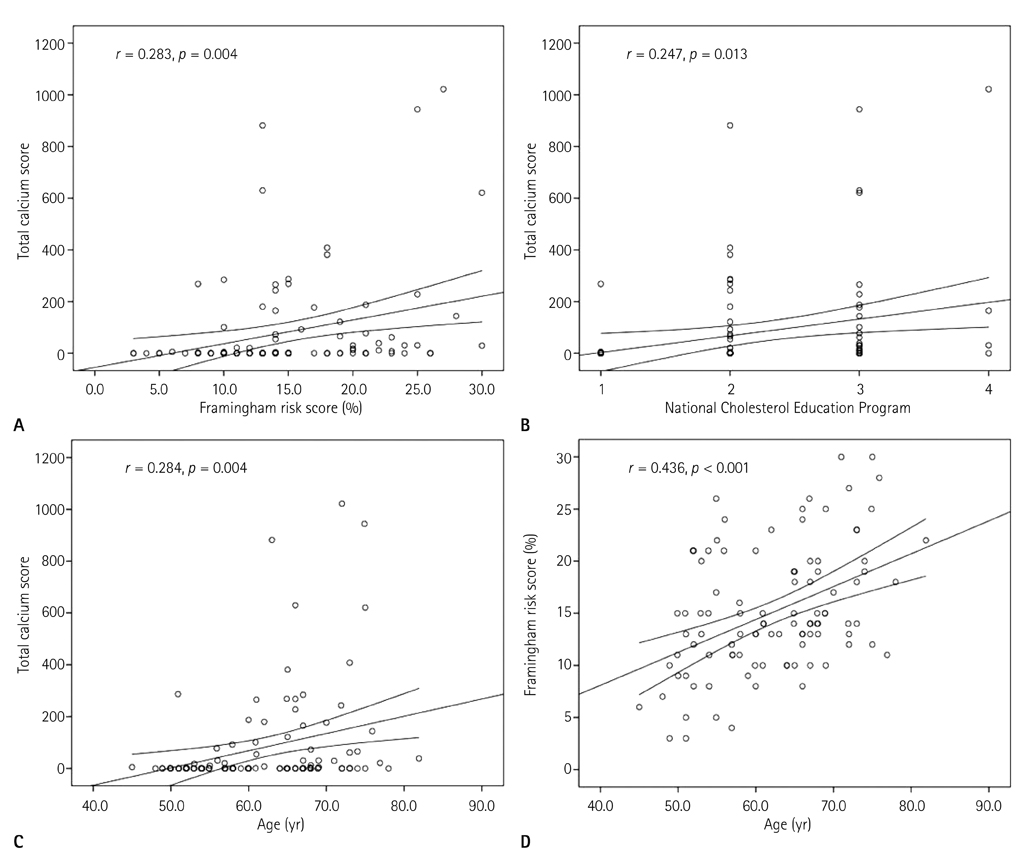
Fig. 1 Scatterplots show that correlation between FRS and TCS (A), between NCEP and TCS (B), between age and TCS (C), between age and FRS (D). TCS was significantly positively correlated with FRS (r = 0.283, p = 0.004) as well as NCEP (r = 0.247, p = 0.013). TCS and FRS significantly increased with age. Note.-FRS = Framingham risk score, NCEP = National Cholesterol Education Program, TCS = total calcium score

Fig. 2 Receiver operating characteristics curve illustrate that coronary artery calcification risk by Framingham risk score (FRS). Area under the curve (AUC) was 0.69 (95% CI, 0.59-0.79) with cutoff point of 13.5%. Note.-CI = confidence interval
Reference
-
1. Korea National Statistical Office. Cause of Death Statistics. cited Dec 1, 2010. Available: http://www.kosis.kr/domestic/theme/do01_index.jsp.2. Grundy SM, Cleeman JI, Merz CN, Brewer HB Jr, Clark LT, Hunninghake DB, et al. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines. J Am Coll Cardiol. 2004. 44:720–732.3. D'Agostino RB Sr, Vasan RS, Pencina MJ, Wolf PA, Cobain M, Massaro JM, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008. 117:743–753.4. Ha EJ, Kim Y, Cheung JY, Shim SS. Coronary artery disease in asymptomatic young adults: its prevalence according to coronary artery disease risk stratification and the CT characteristics. Korean J Radiol. 2010. 11:425–432.5. Arad Y, Goodman KJ, Roth M, Newstein D, Guerci AD. Coronary calcification, coronary disease risk factors, C-reactive protein, and atherosclerotic cardiovascular disease events: the St. Francis Heart Study. J Am Coll Cardiol. 2005. 46:158–165.6. Church TS, Levine BD, McGuire DK, Lamonte MJ, Fitzgerald SJ, Cheng YJ, et al. Coronary artery calcium score, risk factors, and incident coronary heart disease events. Atherosclerosis. 2007. 190:224–231.7. Kim MB, Park WJ, Jang KH, Lee DK, Chae HJ, Moon JD. Comparison of cardiovascular disease risk assessment tools by using coronary CT angiography. Korean J Occup Environ Med. 2010. 22:102–113.8. Lau GT, Ridley LJ, Schieb MC, Brieger DB, Freedman SB, Wong LA, et al. Coronary artery stenoses: detection with calcium scoring, CT angiography, and both methods combined. Radiology. 2005. 235:415–422.9. Choi EK, Choi SI, Rivera JJ, Nasir K, Chang SA, Chun EJ, et al. Coronary computed tomography angiography as a screening tool for the detection of occult coronary artery disease in asymptomatic individuals. J Am Coll Cardiol. 2008. 52:357–365.10. Kim DH, Choi SI, Chun EJ, Chang SA, Choi EK, Chang HJ, et al. Coronary CT angiography: focus on a new algorithm as diagnostic tool in routine clinical practice. J Korean Radiol Soc. 2007. 56:461–472.11. Ko SM, Yi JG, Nam CW, Kim DH. The diagnostic accuracy of the 64-slice multi-detector CT coronary angiography for the assessment of coronary artery stenosis in symptomatic patients. J Korean Radiol Soc. 2008. 59:225–234.12. Budoff MJ, Achenbach S, Blumenthal RS, Carr JJ, Goldin JG, Greenland P, et al. Assessment of coronary artery disease by cardiac computed tomography: a scientific statement from the American Heart Association Committee on Cardiovascular Imaging and Intervention, Council on Cardiovascular Radiology and Intervention, and Committee on Cardiac Imaging, Council on Clinical Cardiology. Circulation. 2006. 114:1761–1791.13. Jung IH, Kim JS, Nam HJ, Kim HS, Kim HK, Park DW, et al. Clinical outcomes according to coronary calcium scores in asymptomatic individuals undergoing coronary CT angiography. Korean J Med. 2010. 78:466–476.14. Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M Jr, Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol. 1990. 15:827–832.15. Shaw LJ, Raggi P, Schisterman E, Berman DS, Callister TQ. Prognostic value of cardiac risk factors and coronary artery calcium screening for all-cause mortality. Radiology. 2003. 228:826–833.16. Greenland P, LaBree L, Azen SP, Doherty TM, Detrano RC. Coronary artery calcium score combined with Framingham score for risk prediction in asymptomatic individuals. JAMA. 2004. 291:210–215.17. Kim Y, Hwang I, Kang HC. The relation of coronary artery calcium scores with Framingham Risk Scores. J Korean Acad Fam Med. 2008. 29:762–767.18. Miller BG, MacCalman L. Cause-specific mortality in British coal workers and exposure to respirable dust and quartz. Occup Environ Med. 2010. 67:270–276.19. Landen DD, Wassell JT, McWilliams L, Patel A. Coal dust exposure and mortality from ischemic heart disease among a cohort of U.S. coal miners. Am J Ind Med. 2011. 54:727–733.20. Chen W, Liu Y, Wang H, Hnizdo E, Sun Y, Su L, et al. Long-term exposure to silica dust and risk of total and cause-specific mortality in Chinese workers: a cohort study. PLoS Med. 2012. 9:e1001206.21. Lee WJ, Seon JR, Ahn BS, Park YS. Findings on chest low-dose CT images of group exposed to inorganic dusts. J Radiol Sci Technol. 2011. 34:305–314.22. Korea Occupational Safety and Health Agency. Risk assessment for the prevention of cardio-cerebrovascular disease at workplace (KOSHA Code H-1-2010). cited Dec 14, 2010. Available: http://www.kosha.net/shdb/code/list.jsp.23. Whitworth JA. World Health Organization. International Society of Hypertension Writing Group. 2003 World Health Organization (WHO)/International Society of Hypertension (ISH) statement on management of hypertension. J Hypertens. 2003. 21:1983–1992.24. Sanders WL. Heart disease and pneumoconiosis. Thorax. 1970. 25:223–225.25. Donaldson K, Stone V, Seaton A, MacNee W. Ambient particle inhalation and the cardiovascular system: potential mechanisms. Environ Health Perspect. 2001. 109:Suppl 4. 523–527.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Relation of Pulmonary Function Impairment and Coronary Artery Calcification by Multi-detector Computed Tomography in Group Exposed to Inorganic Dusts
- The Relationship between Coronary Risk Factors and Coronary Calcium Score Detected by Computed Tomography Coronary Angiography in Korean Middle Aged Men
- Anger and Coronary Calcification in Individuals with and without Risk Factors of Coronary Artery Disease
- Neutrophil-to-Lymphocyte Ratio for Risk Assessment in Coronary Artery Disease and Carotid Artery Atherosclerosis
- Breast Arterial Calcification: A Potential Surrogate Marker for Cardiovascular Disease
