Relation of Pulmonary Function Impairment and Coronary Artery Calcification by Multi-detector Computed Tomography in Group Exposed to Inorganic Dusts
- Affiliations
-
- 1Occupational Lung Diseases Institute, Korea Workers' Compensation and Welfare Service (KCOMWEL), Ansan, Korea. atomlwj@daum.net
Abstract
- BACKGROUND
The purpose of this study was to evaluate the relationship of pulmonary function impairment (PFI) and coronary artery calcification (CAC) by multi-detector computed tomography (MDCT), and the effect of pneumoconiosis on CAC or PFI.
METHODS
Seventy-six subjects exposed to inorganic dusts underwent coronary artery calcium scoring by MDCT, spirometry, laboratory tests, and a standardized questionnaire. CAC was quantified using a commercial software (Rapidia ver. 2.8), and all the subjects were divided into two categories according to total calcium scores (TCSs), either the non-calcified (<1) or the calcified (> or =1) group. Obstructive pulmonary function impairment (OPFI) was defined as forced expiratory volume in one second/forced vital capacity (FEV1/FVC, %)<70, and as FEV1/FVC (%)> or =70 and FVC<80 for restrictive pulmonary function impairment (RPFI) by spirometry. All subjects were classified as either the case (profusion> or =1/0) or the control (profusion< or =0/1) group by pneumoconiosis findings on simple digital radiograph.
RESULTS
Of the 76 subjects, 35 subjects (46.1%) had a CAC. Age and hypertension were different significantly between the non-calcified and the calcified group (p<0.05). Subjects with pneumoconiosis were more frequent in the calcified group than those in the non-calcified group (p=0.099). FEV1/FVC (%) was significantly correlated with TCSs (r=-0.316, p=0.005). Subjects with OPFI tended to increase significantly with increasing of TCS (4.82, p=0.028), but not significantly in RPFI (2.18, p=0.140). Subjects with OPFI were significantly increased in the case group compared to those in the control group.
CONCLUSION
CAC is significantly correlated with OPFI, and CAC and OPFI may be affected by pneumoconiosis findings.
Keyword
MeSH Terms
Figure
-
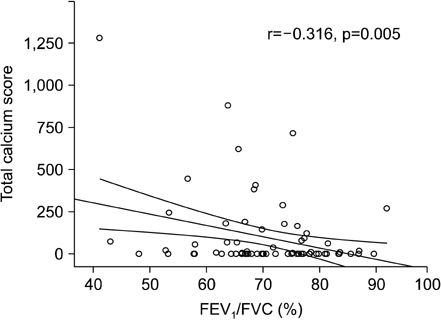
Figure 1 Scatterplot shows that relationship of forced expiratory volume in one second/forced vital capacity (FEV1/FVC, %) and total calcium score. FEV1/FVC (%) was significantly correlated with total calcium score. Pearson's correlation coefficient was -0.316 (p=0.005).

Figure 2 Percentage of subjects with obstructive pulmonary function impairment (OPFI) tended to increase significantly according to the increase of categories of total calcium score (4.82, p=0.028), but not significant in restrictive pulmonary function impairment (RPFI; 2.18, p=0.140), by calculating the linear by linear association of chi-square test. RPFI was defined as forced expiratory volume in one second/forced vital capacity (FEV1/FVC, %) ≥70 and FVC<80, and as FEV1/FVC (%)<70 for OPFI by spirometry.
Reference
-
1. Wexler L, Brundage B, Crouse J, Detrano R, Fuster V, Maddahi J, et al. Writing Group. Coronary artery calcification: pathophysiology, epidemiology, imaging methods, and clinical implications. A statement for health professionals from the American Heart Association. Circulation. 1996. 94:1175–1192.2. Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M Jr, Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol. 1990. 15:827–832.3. Guerci AD, Spadaro LA, Popma JJ, Goodman KJ, Brundage BH, Budoff M, et al. Relation of coronary calcium score by electron beam computed tomography to arteriographic findings in asymptomatic and symptomatic adults. Am J Cardiol. 1997. 79:128–133.4. Arad Y, Goodman KJ, Roth M, Newstein D, Guerci AD. Coronary calcification, coronary disease risk factors, C-reactive protein, and atherosclerotic cardiovascular disease events: the St. Francis Heart Study. J Am Coll Cardiol. 2005. 46:158–165.5. Church TS, Levine BD, McGuire DK, Lamonte MJ, Fitzgerald SJ, Cheng YJ, et al. Coronary artery calcium score, risk factors, and incident coronary heart disease events. Atherosclerosis. 2007. 190:224–231.6. Kim MB, Park WJ, Jang KH, Lee DK, Chae HJ, Moon JD. Comparison of cardiovascular disease risk assessment tools by using coronary CT angiography. Korean J Occup Environ Med. 2010. 22:102–113.7. Rabe KF, Hurd S, Anzueto A, Barnes PJ, Buist SA, Calverley P, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007. 176:532–555.8. Miller BG, MacCalman L. Cause-specific mortality in British coal workers and exposure to respirable dust and quartz. Occup Environ Med. 2010. 67:270–276.9. Landen DD, Wassell JT, McWilliams L, Patel A. Coal dust exposure and mortality from ischemic heart disease among a cohort of U.S. coal miners. Am J Ind Med. 2011. 54:727–733.10. Chen W, Liu Y, Wang H, Hnizdo E, Sun Y, Su L, et al. Long-term exposure to silica dust and risk of total and cause-specific mortality in Chinese workers: a cohort study. PLoS Med. 2012. 9:e1001206.11. Lee WJ, Seon JR, Ahn BS, Park YS. Findings on chest low-dose CT images of group exposed to inorganic dusts. J Radiol Sci Technol. 2011. 34:305–314.12. Topsakal R, Eryol NK, Abaci A, Oymak S, Ozdogru I, Yilmaz Y, et al. The relation between chronic obstructive pulmonary disease and coronary collateral vessels. Angiology. 2005. 56:651–656.13. Fimognari FL, Scarlata S, Conte ME, Incalzi RA. Mechanisms of atherothrombosis in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2008. 3:89–96.14. Topsakal R, Kalay N, Ozdogru I, Cetinkaya Y, Oymak S, Kaya MG, et al. Effects of chronic obstructive pulmonary disease on coronary atherosclerosis. Heart Vessels. 2009. 24:164–168.15. Park HY, Lim SY, Hwang JH, Choi JH, Koh WJ, Sung J, et al. Lung function, coronary artery calcification, and metabolic syndrome in 4905 Korean males. Respir Med. 2010. 104:1326–1335.16. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. Eur Respir J. 2005. 26:319–338.17. Jung IH, Kim JS, Nam HJ, Kim HS, Kim HK, Park DW, et al. Clinical outcomes according to coronary calcium scores in asymptomatic individuals undergoing coronary CT angiography. Korean J Med. 2010. 78:466–476.18. Mehta AJ, Miedinger D, Keidel D, Bettschart R, Bircher A, Bridevaux PO, et al. Occupational exposure to dusts, gases, and fumes and incidence of chronic obstructive pulmonary disease in the Swiss Cohort Study on Air Pollution and Lung and Heart Diseases in Adults. Am J Respir Crit Care Med. 2012. 185:1292–1300.19. Lee JO, Choi BS, Lee JS, Jeong JY, Lee HK. Annual changes of lung function in retired workers exposed to inorganic dusts. Tuberc Respir Dis. 2011. 71:341–348.20. Lee JO, Lee YL, Choi BS, Lee HK. The application of impulse oscillometry (IOS) in the workers who had been exposed to inorganic dust induced early airway obstruction. Tuberc Respir Dis. 2011. 71:431–437.21. Donaldson K, Stone V, Seaton A, MacNee W. Ambient particle inhalation and the cardiovascular system: potential mechanisms. Environ Health Perspect. 2001. 109:Suppl 4. 523–527.22. Lee WJ, Lee JO, Choi BS. Evaluation of obstructive pulmonary function impairment risks in pulmonary emphysema detected by low-dose CT: compared with simple digital radiography. Tuberc Respir Dis. 2011. 71:37–45.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Three cases of right coronary anomaly confirmed by multi-detector computed tomography
- Unusual Coronary Artery Fistula: Left Anterior Descending Coronary Artery - Left Ventricular Fistula Diagnosed by ECG-Gated Multi-Detector Row Coronary CT Angiography
- Relationship between Conventional Cardiovascular Disease Risk Assessment and Coronary Artery Calcification in Group Exposed to Inorganic Dusts
- Spectrum of Multi-Detector Computed Tomography Findings that Alter Pulmonary Artery Diameters in Adults
- Overlooked or unrecognized pitfalls in noninvasive multi-detector computed tomography coronary angiography
