Implications of Emphysema and Lung Function for the Development of Pneumonia in Patients with Chronic Obstructive Pulmonary Disease
- Affiliations
-
- 1Department of Internal Medicine, Kangwon National University Hospital, Kangwon National University College of Medicine, Chuncheon, Korea.
- 2Department of Pulmonary and Critical Care Medicine and Clinical Research Center for Chronic Obstructive Airway Diseases, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. ymoh55@amc.seoul.kr
- 3Department of Internal Medicine, Konkuk University School of Medicine, Seoul, Korea.
- 4Department of Internal Medicine, CHA Bundang Medical Center, CHA University, Seongnam, Korea.
- 5Division of Pulmonary and Critical Care Medicine, Department of Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 6Department of Internal Medicine, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- KMID: 2320771
- DOI: http://doi.org/10.4046/trd.2016.79.2.91
Abstract
- BACKGROUND
Chronic obstructive pulmonary disease (COPD) is sometimes complicated with pneumonia, but little is known about the risk factors that promote the development of pneumonia in COPD. These risk factors were evaluated in the present study.
METHODS
The data of 324 patients with COPD from a prospective multi-center observational cohort with obstructive lung disease were evaluated retrospectively. To identify risk factors for the development of pneumonia in COPD, the clinical and radiological data at enrollment and the time to the first episode of pneumonia were analyzed by Cox proportional hazard analysis.
RESULTS
The median follow-up time was 1,099 days and 28 patients (8.6%) developed pneumonia. The Cox analysis showed that post-bronchodilator forced expiratory volume in one second (FEV1, % of predicted) and the computed tomography (CT) emphysema extent (inspiratory V950) were independent risk factors for the development of pneumonia (post-bronchodilator FEV1: hazard ratio [HR], 0.97; 95% confidence interval [CI], 0.94-1.00; p=0.048 and inspiratory V950: HR, 1.04; 95% CI, 1.01-1.07; p=0.01).
CONCLUSION
Emphysema severity measured by CT and post-bronchodilator FEV1 are important risk factors for the development of pneumonia in COPD.
Keyword
MeSH Terms
Figure
-
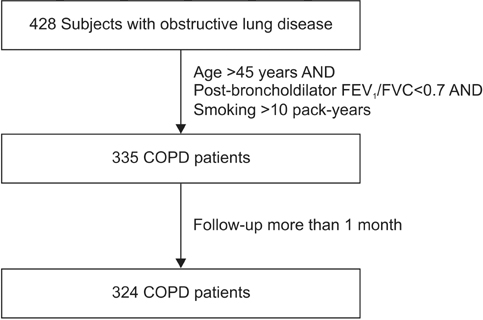
Figure 1 Selection of study subjects from the initial cohort with obstructive lung disease. FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; COPD: chronic obstructive pulmonary disease.

Figure 2 Kaplan-Meier plot showing the development of pneumonia over time in the patient groups with mild, moderate, and severe emphysema extent, as determined by computed tomography (CT). The patients were classified into three groups on the basis of emphysema extent, as indicated by the CT measurement of inspiratory volume fraction (%) of the lung below –950 Hounsfield unit (V950). The patients in the 33th percentile or less, the 34th to 66th percentile, and the 67th percentile or greater were categorized as having mild, moderate, and severe emphysema, respectively. Logrank (Mantel-Cox) test, p<0.001.
Reference
-
1. Han MK, Agusti A, Calverley PM, Celli BR, Criner G, Curtis JL, et al. Chronic obstructive pulmonary disease phenotypes: the future of COPD. Am J Respir Crit Care Med. 2010; 182:598–604.2. Mannino DM, Buist AS. Global burden of COPD: risk factors, prevalence, and future trends. Lancet. 2007; 370:765–773.3. Centers for Disease Control and Prevention (CDC). Pneumonia and influenza death rates: United States, 1979-1994. MMWR Morb Mortal Wkly Rep. 1995; 44:535–537.4. Falguera M, Martin M, Ruiz-Gonzalez A, Pifarre R, Garcia M. Community-acquired pneumonia as the initial manifestation of serious underlying diseases. Am J Med. 2005; 118:378–383.5. Mannino DM, Davis KJ, Kiri VA. Chronic obstructive pulmonary disease and hospitalizations for pneumonia in a US cohort. Respir Med. 2009; 103:224–229.6. Molinos L, Clemente MG, Miranda B, Alvarez C, del Busto B, Cocina BR, et al. Community-acquired pneumonia in patients with and without chronic obstructive pulmonary disease. J Infect. 2009; 58:417–424.7. Pifarre R, Falguera M, Vicente-de-Vera C, Nogues A. Characteristics of community-acquired pneumonia in patients with chronic obstructive pulmonary disease. Respir Med. 2007; 101:2139–2144.8. Calverley PM, Stockley RA, Seemungal TA, Hagan G, Willits LR, Riley JH, et al. Reported pneumonia in patients with COPD: findings from the INSPIRE study. Chest. 2011; 139:505–512.9. Calverley PM, Anderson JA, Celli B, Ferguson GT, Jenkins C, Jones PW, et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007; 356:775–789.10. Drummond MB, Dasenbrook EC, Pitz MW, Murphy DJ, Fan E. Inhaled corticosteroids in patients with stable chronic obstructive pulmonary disease: a systematic review and meta-analysis. JAMA. 2008; 300:2407–2416.11. Singh S, Amin AV, Loke YK. Long-term use of inhaled corticosteroids and the risk of pneumonia in chronic obstructive pulmonary disease: a meta-analysis. Arch Intern Med. 2009; 169:219–229.12. Han MK, Kazerooni EA, Lynch DA, Liu LX, Murray S, Curtis JL, et al. Chronic obstructive pulmonary disease exacerbations in the COPDGene study: associated radiologic phenotypes. Radiology. 2011; 261:274–282.13. Kim WJ, Oh YM, Sung J, Lee YK, Seo JB, Kim N, et al. CT scanning-based phenotypes vary with ADRB2 polymorphisms in chronic obstructive pulmonary disease. Respir Med. 2009; 103:98–103.14. Fishman A, Martinez F, Naunheim K, Piantadosi S, Wise R, Ries A, et al. A randomized trial comparing lung-volume-reduction surgery with medical therapy for severe emphysema. N Engl J Med. 2003; 348:2059–2073.15. Kim WJ, Oh YM, Sung J, Kim TH, Huh JW, Jung H, et al. Lung function response to 12-week treatment with combined inhalation of long-acting beta2 agonist and glucocorticoid according to ADRB2 polymorphism in patients with chronic obstructive pulmonary disease. Lung. 2008; 186:381–386.16. Quan H, Li B, Couris CM, Fushimi K, Graham P, Hider P, et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol. 2011; 173:676–682.17. Lee YK, Oh YM, Lee JH, Kim EK, Lee JH, Kim N, et al. Quantitative assessment of emphysema, air trapping, and airway thickening on computed tomography. Lung. 2008; 186:157–165.18. Almirall J, Bolibar I, Serra-Prat M, Palomera E, Roig J, Hospital I, et al. Relationship between the use of inhaled steroids for chronic respiratory diseases and early outcomes in community-acquired pneumonia. PLoS One. 2013; 8:e73271.19. Eom JS, Song WJ, Yoo H, Jeong BH, Lee HY, Koh WJ, et al. Chronic obstructive pulmonary disease severity is associated with severe pneumonia. Ann Thorac Med. 2015; 10:105–111.20. Han MK, Bartholmai B, Liu LX, Murray S, Curtis JL, Sciurba FC, et al. Clinical significance of radiologic characterizations in COPD. COPD. 2009; 6:459–467.21. Martinez FJ, Foster G, Curtis JL, Criner G, Weinmann G, Fishman A, et al. Predictors of mortality in patients with emphysema and severe airflow obstruction. Am J Respir Crit Care Med. 2006; 173:1326–1334.22. Kim V, Han MK, Vance GB, Make BJ, Newell JD, Hokanson JE, et al. The chronic bronchitic phenotype of COPD: an analysis of the COPDGene Study. Chest. 2011; 140:626–633.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical use of chest CT in chronic obstructive pulmonary diseases
- Pathophysiology of Chronic Obstructive Pulmonary Disease
- Pathophysiology of Chronic Obstructive Pulmonary Disease
- Clinical Applications of Bronchoscopic Lung Volume Reduction for Patients with Severe Emphysema
- Quantification of Emphysema with a Three-Dimensional Chest CT Scan: Correlation with the Visual Emphysema Scoring on Chest CT, Pulmonary Function Tests and Dyspnea Severity
