A Case of Pulmonary Cryptococcosis in an Immunocompetent Male Patient Diagnosed by a Percutaneous Supraclavicular Lymph Node Biopsy
- Affiliations
-
- 1Department of Internal Medicine, Bundang Jesaeng General Hospital, Seongnam, Korea. dhkim@dmc.or.kr
- 2Department of Radiology, Bundang Jesaeng General Hospital, Seongnam, Korea.
- 3Department of Pathology, Bundang Jesaeng General Hospital, Seongnam, Korea.
- KMID: 2320656
- DOI: http://doi.org/10.4046/trd.2015.78.3.276
Abstract
- Cryptococcal pneumonia usually occurs in immunocompromised patients with malignancy, acquired immune deficiency syndrome, organ transplantations, immunosuppressive chemotherapies, catheter insertion, or dialysis. It can be diagnosed by gaining tissues in lung parenchyma or detecting antigen in blood or bronchoalveolar lavage fluid. Here we report an immunocompetent 32-year-old male patient with diabetes mellitus diagnosed with cryptococcal pneumonia after a ultrasound-guided percutaneous supraclavicular lymph node core needle biopsy. We treated him with fluconazole at 400 mg/day for 9 months according to the guideline. This is the first case that cryptococcal pneumonia was diagnosed from a percutaneous lymph node biopsy in South Korea.
Keyword
MeSH Terms
Figure
-

Figure 1 Initial lung images. (A) Initial chest radiograph showing diffuse reticulonodular opacities in both lungs. (B) Initial chest computed tomography (CT) scan shows innumerable small nodules, interstitial thickening, and ground glass attenuation in both lungs. Note small bilateral pleural effusions. Both hilar regions are enlarged, representing lymphadenopathy. (C) Chest CT mediastinal window setting coronal image showing enlarged lymph nodes in both supraclavicular areas, both mediastinal, interlobar, and subcarinal areas.

Figure 2 Supraclavicular lymph node biopsy. (A) Granulomatous inflammation in cryptococcosis showing numerous multinucleated giant cells (H&E stain). (B) The periodic acid-Schiff stain reveals yeast forms of Cryptococcus separated from the cell cytoplasm by a clear space. (C) The capsule of Cryptococcus stained bright-red with mucicarmine stain (A, ×100; B and C, ×400).
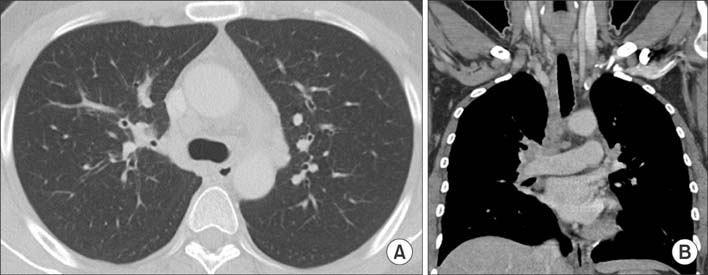
Figure 3 Three-month follow-up lung images. (A) Chest computed tomography (CT) scan showing markedly improved small nodules in both lungs after treatment with fluconazole for 3 months. (B) Chest CT scan showing improved lymphadenopathy noted on initial chest CT scan.

Figure 4 Lung images at 9-month follow-up. (A) Chest computed tomography (CT) scan showing no cryptococcosis related lesion. (B) Chest CT scan showing no lymphadenopathy.
Reference
-
1. Chang WC, Tzao C, Hsu HH, Lee SC, Huang KL, Tung HJ, et al. Pulmonary cryptococcosis: comparison of clinical and radiographic characteristics in immunocompetent and immunocompromised patients. Chest. 2006; 129:333–340.2. Nadrous HF, Antonios VS, Terrell CL, Ryu JH. Pulmonary cryptococcosis in nonimmunocompromised patients. Chest. 2003; 124:2143–2147.3. Nakamura S, Miyazaki Y, Higashiyama Y, Yanagihara K, Ohno H, Hirakata Y, et al. Community acquired pneumonia (CAP) caused by Cryptococcus neoformans in a healthy individual. Scand J Infect Dis. 2005; 37:932–935.4. Chang YS, Chou KC, Wang PC, Yang HB, Chen CH. Primary pulmonary cryptococcosis presenting as endobronchial tumor with left upper lobe collapse. J Chin Med Assoc. 2005; 68:33–36.5. Smith JA, Kauffman CA. Pulmonary fungal infections. Respirology. 2012; 17:913–926.6. Perfect JR, Dismukes WE, Dromer F, Goldman DL, Graybill JR, Hamill RJ, et al. Clinical practice guidelines for the management of cryptococcal disease: 2010 update by the infectious diseases society of america. Clin Infect Dis. 2010; 50:291–322.7. Huang L, Crothers K. HIV-associated opportunistic pneumonias. Respirology. 2009; 14:474–485.8. Johannson KA, Huston SM, Mody CH, Davidson W. Cryptococcus gattii pneumonia. CMAJ. 2012; 184:1387–1390.9. Thomas CJ, Lee JY, Conn LA, Bradley ME, Gillespie RW, Dill SR, et al. Surveillance of cryptococcosis in Alabama, 1992-1994. Ann Epidemiol. 1998; 8:212–216.10. Saag MS, Graybill RJ, Larsen RA, Pappas PG, Perfect JR, Powderly WG, et al. Practice guidelines for the management of cryptococcal disease. Infectious Diseases Society of America. Clin Infect Dis. 2000; 30:710–718.11. Fox DL, Muller NL. Pulmonary cryptococcosis in immunocompetent patients: CT findings in 12 patients. AJR Am J Roentgenol. 2005; 185:622–626.12. Lindell RM, Hartman TE, Nadrous HF, Ryu JH. Pulmonary cryptococcosis: CT findings in immunocompetent patients. Radiology. 2005; 236:326–331.13. Hung MS, Tsai YH, Lee CH, Yang CT. Pulmonary cryptococcosis: clinical, radiographical and serological markers of dissemination. Respirology. 2008; 13:247–251.14. Guy JP, Raza S, Bondi E, Rosen Y, Kim DS, Berger BJ. Cryptococcus pneumonia presenting in an immunocompetent host with pulmonary asbestosis: a case report. J Med Case Rep. 2012; 6:170.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Massive Mediastinal Lymph Node Involvement of Cryptococcosis in Immunocompetent Host
- Cryptococcosis with Mediastinal Lymph Node and Lung Involvement in an Immunocompetent Adolescent: A Case Report
- A Case of Pulmonary Cryptococcosis Mimicking Bronchogenic Lung Cancer in an Immunocompetent Patient: A Review of the Literature
- Supraclavicular Lymph Node Excision Biopsy in Patients with Suspected Supraclavicular Lymph Node Metastasis of Lung Cancer: Experience in a Tertiary Hospital
- Pulmonary Cryptococcosis in Immunocompetent Patients: CT Findings
