Two Cases of Diagnosis and Removal of Endobronchial Hamartoma by Cryotherapy via Flexible Bronchoscopy
- Affiliations
-
- 1Division of Respiratory and Critical Care Medicine, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea. minkyunghoon@korea.ac.kr
Abstract
- Although endobronchial hamartoma is a rare benign tumor, most patients with endobronchial hamartoma have respiratory symptoms such as obstructive pneumonia, hemoptysis, cough, or dyspnea due to bronchial obstruction. It can cause irreversible post-obstructive pulmonary destruction, thus early diagnosis and treatment is very important. Recently, there have been cases of neodymium-doped yttrium aluminum garnet (Nd:YAG) laser and electrocautery procedures for bronchoscopic treatment of malignant or benign central airway obstruction with comparable therapeutic efficacy and few complications. Bronchoscopic cryotherapy is a newly developed technique for management of central airway obstruction. Moreover, it provides diagnostic methods with improving diagnostic yield and safety. We report two cases of endobronchial hamartoma, each diagnosed and definitively treated with bronchoscopic techniques. Endobronchial biopsy and removal was successfully performed by cryotherapy via flexible bronchoscopy without notable complications. Follow-up bronchoscopic examinations excluded residual or recurrent disease.
Keyword
MeSH Terms
Figure
-

Figure 1 (A-D) Imaging study on admission day suggested obstructive pneumonia on superior segment of right lower lung (RS6). (A, B) Posterior-anterior (PA) view and lateral view of chest X-ray. (C) Transverse section of chest computed tomography (CT). (D) Coronal section of chest CT. (E-H) Imaging study at 3 months after removal of endobronchial hamartoma on superior segmental bronchus of right lower lung (RB6) showed completely resolution of previous obstructive pneumonia on RS6. (E, F) PA view and lateral view of chest X-ray. (G) Transverse section of chest CT. (H) Coronal section of chest CT.
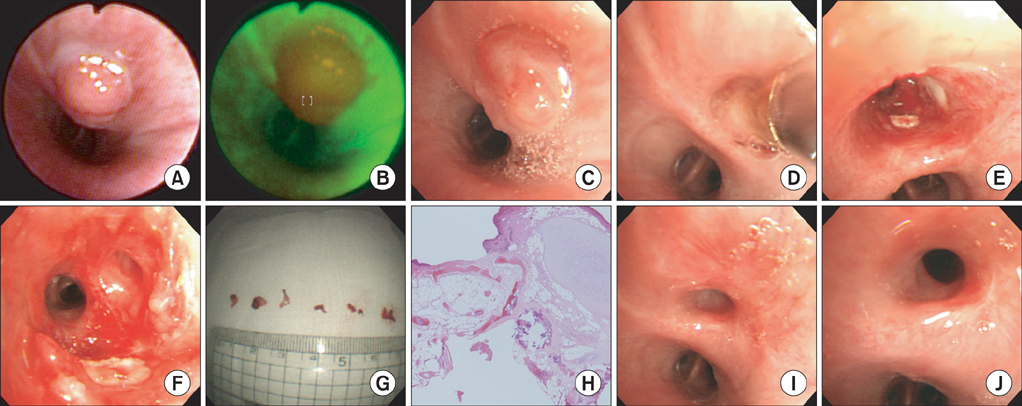
Figure 2 (A, B) The bronchoscopic examination showed the superior segmental bronchus of right lower lung (RB6) was obstructed by pedunculated mass. (A) White light image. (B) Autofluorescence image. (C-G) Procedure image of resection of the mass on RB6 with cryotherapy. Biopsy showed chondroid hamartoma (H&E stain, ×100) (H) and bronchoscopic examination after 3 months after resection of endobronchial hamartoma showed good patency without any obstruction of RB6 (I, J).

Figure 3 (A-C) Imaging study of personal health examination showed a 1.1 cm-sized fat density lesion on superior segmental bronchus of left lower lung (LB6). (A) Posterior-anterior (PA) view of chest X-ray. (B) Transverse section of chest computed tomography (CT). (C) Coronal section of chest CT. (D, E) Imaging study at 1 month after resection of endobronchial hamartoma on LB6. (D) PA view of chest X-ray. (E) Lateral view of chest X-ray.

Figure 4 (A, B) The bronchoscopic examination showed the superior segmental bronchus of left lower lung (LB6) was obstructed by pedunculated mass. (A) White light image. (B) Autofluorescence image. (C-G) Procedure image of resection of the mass on LB6 with cryotherapy. Biopsy showed hamartoma (H&E stain, ×100) (H) and bronchoscopic examination after 1 month after resection of endobronchial hamartoma showed good patency without any obstruction of LB6 (I, J).
Reference
-
1. Miller SM, Bellinger CR, Chatterjee A. Argon plasma coagulation and electrosurgery for benign endobronchial tumors. J Bronchology Interv Pulmonol. 2013; 20:38–40.2. Mathur PN, Wolf KM, Busk MF, Briete WM, Datzman M. Fiberoptic bronchoscopic cryotherapy in the management of tracheobronchial obstruction. Chest. 1996; 110:718–723.3. Maiwand MO, Asimakopoulos G. Cryosurgery for lung cancer: clinical results and technical aspects. Technol Cancer Res Treat. 2004; 3:143–150.4. Murray J, Kielkowski D, Leiman G. The prevalence and age distribution of peripheral pulmonary hamartomas in adult males: an autopsy-based study. S Afr Med J. 1991; 79:247–249.5. Gjevre JA, Myers JL, Prakash UB. Pulmonary hamartomas. Mayo Clin Proc. 1996; 71:14–20.6. Lee SH, Yoon HK, Song SH, Lee SY, Kim SC, Ahn JH, et al. Clinical analysis of pulmonary hamartoma: 29 cases. Tuberc Respir Dis. 2002; 53:644–649.7. Kim SA, Um SW, Song JU, Jeon K, Koh WJ, Suh GY, et al. Bronchoscopic features and bronchoscopic intervention for endobronchial hamartoma. Respirology. 2010; 15:150–154.8. Cosio BG, Villena V, Echave-Sustaeta J, de Miguel E, Alfaro J, Hernandez L, et al. Endobronchial hamartoma. Chest. 2002; 122:202–205.9. Sunna R. Chapter 33. Cryotherapy and cryodebridement. In : Ernst A, Herth FJ, editors. Principles and practice of interventional pulmonology. New York: Springer Science;2013. p. 343–350.10. Morgan RK, Ernst A. Chapter 12. Cryotherapy. In : Strausz J, Bolliger CT, editors. Interventional pulmonology: European respiratory monograph. Sheffield: European Respiratory Society;2010. p. 161–172.11. Ernst A, Feller-Kopman D, Becker HD, Mehta AC. Central airway obstruction. Am J Respir Crit Care Med. 2004; 169:1278–1297.12. Vergnon JM, Huber RM, Moghissi K. Place of cryotherapy, brachytherapy and photodynamic therapy in therapeutic bronchoscopy of lung cancers. Eur Respir J. 2006; 28:200–218.13. Schumann C, Hetzel J, Babiak AJ, Merk T, Wibmer T, Moller P, et al. Cryoprobe biopsy increases the diagnostic yield in endobronchial tumor lesions. J Thorac Cardiovasc Surg. 2010; 140:417–421.14. Babiak A, Hetzel J, Krishna G, Fritz P, Moeller P, Balli T, et al. Transbronchial cryobiopsy: a new tool for lung biopsies. Respiration. 2009; 78:203–208.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endobronchial hamartoma treated bronchoscopically: Report of two cases
- A Case of Endobronchial Actinomycosis with a Broncholith cured by Cryotherapy through a Flexible Bronchoscope
- Endoscopic Cryosurgical Resection of Pulmonary Hamartoma with Flexible Bronchoscopy
- Successful Removal of Endobronchial Blood Clots Using Bronchoscopic Cryotherapy at Bedside in the Intensive Care Unit
- A Case of Endobronchial Hamartoma Diagnosed by Fiberoptic Bronchoscopy
