Successful Rechallenge with Imatinib in a Patient with Chronic Myeloid Leukemia Who Previously Experienced Imatinib Mesylate Induced Pneumonitis
- Affiliations
-
- 1Department of Internal Medicine, The Catholic University of Korea College of Medicine, Seoul, Korea. rkdwldud@catholic.ac.kr
- 2Department of Pathology, The Catholic University of Korea College of Medicine, Seoul, Korea.
Abstract
- Imatinib mesylate is a targeted therapy that acts by inhibiting tyrosine kinase of the bcr-abl fusion oncoprotein, which is specific to chronic myeloid leukemia (CML), and the c-transmembrane receptor, which is specific to gastrointestinal stromal tumors. Interstitial pneumonitis is a rare adverse event of imatinib therapy. It is clinically difficult to distinguish from infectious pneumonia, which can frequently occur due to the underlying disease. The standard treatment for imatinib-induced pneumonitis is to discontinue the medication and optionally administer corticosteroids. However, there are a few cases of successful retrial with imatinib. We describe a case of successful rechallenge of imatinib in a patient with imatinib-induced interstitial pneumonitis and CML without a recurrence of the underlying disease after 3 months of follow-up.
MeSH Terms
Figure
-
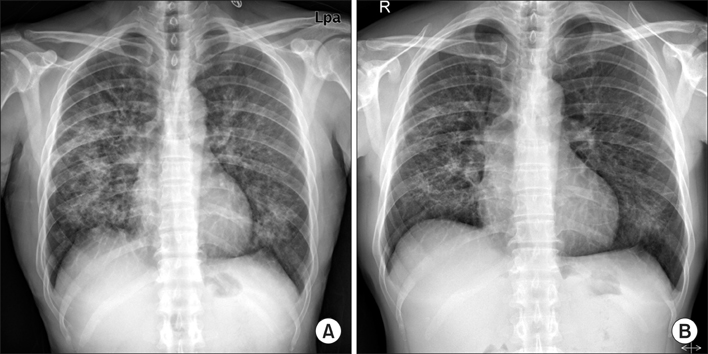
Figure 1 Chest X-ray shows bilateral reticulonodular infiltration in both lungs at admission (A) and slight regression of peribronchial patchy opacities in both lungs at 2 weeks after discontinuing imatinib and commencing steroid treatment (B).

Figure 2 Chest high resolution computed tomography scan reveals patchy ground glass opacities with some interlobar and intralobular septal thickening in both lungs, predominantly seen in the central and upper lung zones (A), and interval improvement of the interstitial pneumonia with some remaining ground glass opacity after 12 weeks of rechallenge with imatinib (B).

Figure 3 (A, B) Transbronchial lung biopsy specimen reveals organizing pattern of interstitial pneumonia, showing fibroblastic plug formation in the alveoli with infiltration of chronic inflammatory cells and mild fibrous thickening in the interstitium (H&E stain; A, ×40; B, ×200).
Reference
-
1. Deininger MW, Goldman JM, Melo JV. The molecular biology of chronic myeloid leukemia. Blood. 2000; 96:3343–3356.2. Ohnishi K, Sakai F, Kudoh S, Ohno R. Twenty-seven cases of drug-induced interstitial lung disease associated with imatinib mesylate. Leukemia. 2006; 20:1162–1164.3. Kim TH, Kim BG, Cho SW, Cho SK, Kim HJ, Yuh YJ, et al. Imatinib-mesylate induced interstitial pneumonitis in two CML patients. Tuberc Respir Dis. 2011; 71:210–215.4. Lee JW, Kim HJ, Kim KJ, Shin KC, Hong YH, Chung JH, et al. A case of imatinib-mesylate associated hypersensitivity pneumonitis. Tuberc Respir Dis. 2005; 59:423–426.5. Barber NA, Ganti AK. Pulmonary toxicities from targeted therapies: a review. Target Oncol. 2011; 6:235–243.6. Yokoyama T, Miyazawa K, Kurakawa E, Nagate A, Shimamoto T, Iwaya K, et al. Interstitial pneumonia induced by imatinib mesylate: pathologic study demonstrates alveolar destruction and fibrosis with eosinophilic infiltration. Leukemia. 2004; 18:645–646.7. Snyder LS, Hertz MI, Peterson MS, Harmon KR, Marinelli WA, Henke CA, et al. Acute lung injury: pathogenesis of intraalveolar fibrosis. J Clin Invest. 1991; 88:663–673.8. Walsh J, Absher M, Kelley J. Variable expression of plateletderived growth factor family proteins in acute lung injury. Am J Respir Cell Mol Biol. 1993; 9:637–644.9. Rossi SE, Erasmus JJ, McAdams HP, Sporn TA, Goodman PC. Pulmonary drug toxicity: radiologic and pathologic manifestations. Radiographics. 2000; 20:1245–1259.10. Seki N, Ito A, Watanabe K, Shibakuki R, Seto T, Uematsu K, et al. Irreversible imatinib-induced pneumonitis following longterm imatinib administration. Intern Med. 2007; 46:1941–1942.11. Delomas T, Darne C, Besson C. Lack of recurrence of imatinib-induced interstitial lung disease with nilotinib. Leuk Lymphoma. 2012; 53:332–333.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Imatinib-Mesylate Induced Interstitial Pneumonitis in Two CML Patients
- A Case of Drug Eruption with Localized ExfoliativeDermatitis Induced by Imatinib Mesylate
- Peripheral neuropathy associated with imatinib therapy for chronic myeloid leukemia
- Complete remission of philadelphia chromosome-positive acute myeloid leukemia with imatinib mesylate
- A Case of Lichenoid Drug Eruption Associated with Imatinib Mesylate
