Severe Acute Fibrinous and Organizing Pneumonia with Acute Respiratory Distress Syndrome
- Affiliations
-
- 1Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine and Lung Institute, Seoul National University College of Medicine, Seoul, Korea.
- 2Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine and Lung Institute, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea. lungdrcho@gmail.com
Abstract
- Acute fibrinous and organizing pneumonia is a newly recognized pattern of acute lung injury. A 49-year-old female presented with a cough and worsening dyspnea on exertion. She had no history of smoking and no specific past medical history except exposure of home humidifier containing sterilizer. A chest computed tomography scan showed patchy consolidation with fibrosis in the right lower lobe and ill-defined centrilobular ground glass opacity in both lungs. The pathological findings were patchy areas of lung parenchyma with fibrin deposits in the alveolar ducts and alveoli, and fibrin balls with hemosiderin deposition in the alveolar spaces. The histological pattern of our case is differentiated from diffuse alveolar damage by the absence of hyaline membranes, and from eosinophilic pneumonia by the lack of eosinophils. In our case, the patient was treated with corticosteroid pulse therapy. However, the clinical course became aggravated and she died within two weeks.
MeSH Terms
Figure
-
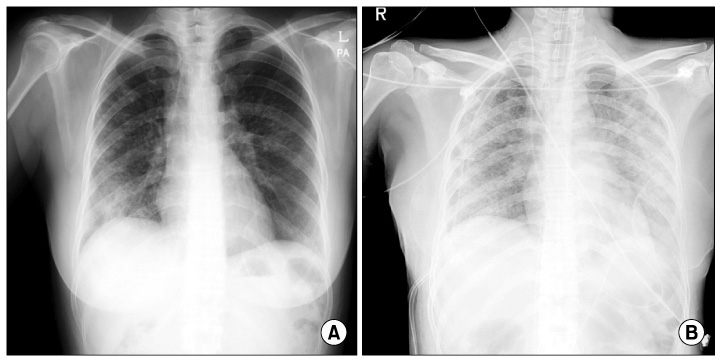
Figure 1 The chest radiography. (A) The initial chest radiography showed diffuse fine reticular and nodular opacities in both lungs. (B) Chest radiography after intubation and application of mechanical ventilation revealed the progression of bilateral nodular opacities and diffuse consolidation.
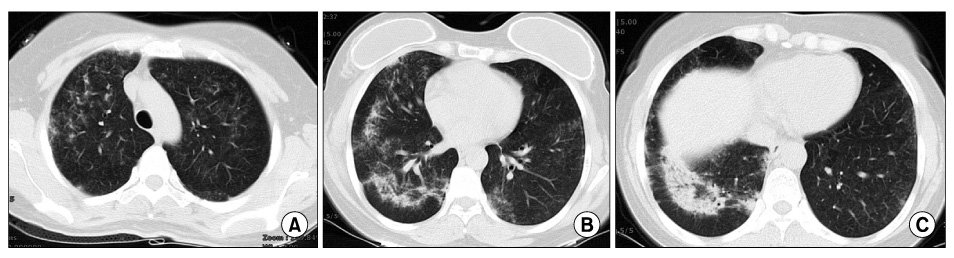
Figure 2 Chest computed tomography scan. (A) Upper lung field, (B) middle lung field and (C) lower lung field. The CT scan showed patchy consolidation with fibrosis in the right lower lobe and ill-defined centrilobular ground glass opacity in the both lungs. CT: computed tomography.
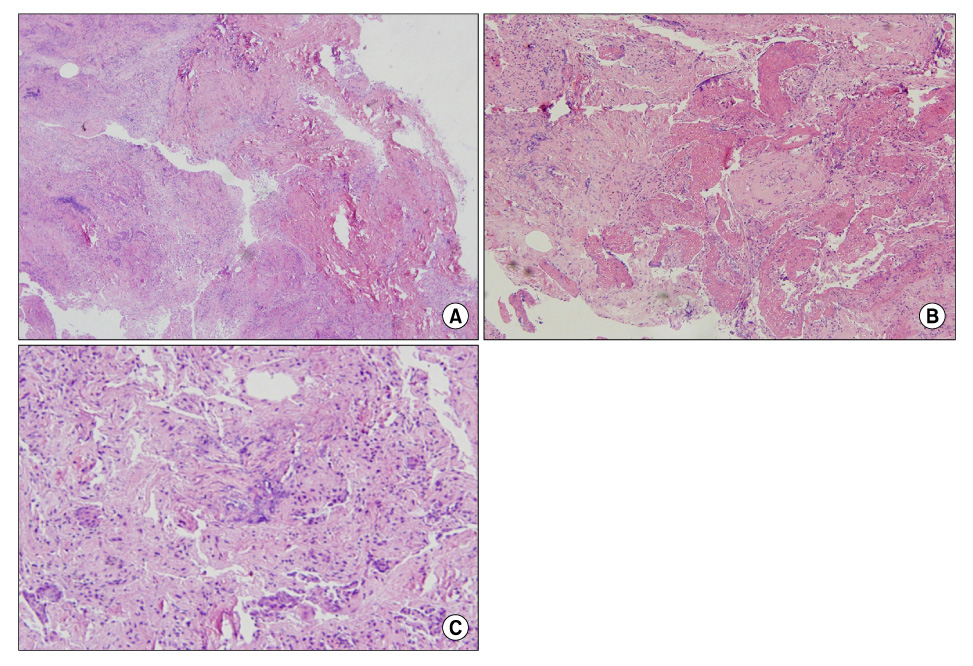
Figure 3 Pathological findings of lung specimens. (A) The biopsy specimen of the lung showed patchy areas of lung parenchymal by fibrin deposits in the alveolar ducts and alveoli (H&E, ×40). (B) The biopsied lung showed that the intra-alveolar spaces contained fibrous plugging with extensive fibrin deposition, a finding consistent with cryptogenic organizing pneumonia with fibrous exudates (H&E, ×100). (C) Fibrin balls with hemosiderin deposition were noted in the alveolar spaces (H&E, ×200).
Reference
-
1. Beasley MB. The pathologist's approach to acute lung injury. Arch Pathol Lab Med. 2010. 134:719–727.2. Beasley MB, Franks TJ, Galvin JR, Gochuico B, Travis WD. Acute fibrinous and organizing pneumonia: a histological pattern of lung injury and possible variant of diffuse alveolar damage. Arch Pathol Lab Med. 2002. 126:1064–1070.3. Damas C, Morais A, Moura CS, Marques A. Acute fibrinous and organizing pneumonia. Rev Port Pneumol. 2006. 12:615–620.4. Balduin R, Giacometti C, Saccarola L, Marulli G, Rea F, Bartoli M, et al. Acute fibrinous and organizing pneumonia in a patient with collagen vascular disease "stigma". Sarcoidosis Vasc Diffuse Lung Dis. 2007. 24:78–80.5. Prahalad S, Bohnsack JF, Maloney CG, Leslie KO. Fatal acute fibrinous and organizing pneumonia in a child with juvenile dermatomyositis. J Pediatr. 2005. 146:289–292.6. Yokogawa N, Alcid DV. Acute fibrinous and organizing pneumonia as a rare presentation of abacavir hypersensitivity reaction. AIDS. 2007. 21:2116–2117.7. Heo JY, Song JY, Noh JY, Yong HS, Cheong HJ, Kim WJ. Acute fibrinous and organizing pneumonia in a patient with HIV infection and Pneumocystis jiroveci pneumonia. Respirology. 2010. 15:1259–1261.8. Lee SM, Park JJ, Sung SH, Kim Y, Lee KE, Mun YC, et al. Acute fibrinous and organizing pneumonia following hematopoietic stem cell transplantation. Korean J Intern Med. 2009. 24:156–159.9. Hariri LP, Unizony S, Stone J, Mino-Kenudson M, Sharma A, Matsubara O, et al. Acute fibrinous and organizing pneumonia in systemic lupus erythematosus: a case report and review of the literature. Pathol Int. 2010. 60:755–759.10. Daftary AS, Deterding RR. Inhalational lung injury associated with humidifier "white dust". Pediatrics. 2011. 127:e509–e512.11. Patterson R, Mazur N, Roberts M, Scarpelli D, Semerdjian R, Harris KE. Hypersensitivity pneumonitis due to humidifier disease: seek and ye shall find. Chest. 1998. 114:931–933.12. Baur X, Behr J, Dewair M, Ehret W, Fruhmann G, Vogelmeier C, et al. Humidifier lung and humidifier fever. Lung. 1988. 166:113–124.13. Müller-Wening D, Koschel D, Stark W, Sennekamp HJ. Humidifier-associated disease in the general population. Dtsch Med Wochenschr. 2006. 131:491–496.14. Bhatti S, Hakeem A, Torrealba J, McMahon JP, Meyer KC. Severe acute fibrinous and organizing pneumonia (AFOP) causing ventilatory failure: successful treatment with mycophenolate mofetil and corticosteroids. Respir Med. 2009. 103:1764–1767.15. Cho JY, Lee HK, Lee SS, Lee HK, Lee YM, Lee HP, et al. A case of acute fibrinous and organizing pneumonia. Tuberc Respir Dis. 2006. 61:479–483.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Acute Fibrinous and Organizing Pneumonia
- Two cases of acute fibrinous and organizing pneumonia
- Acute Eosinophilic Pneumonia
- Acute Fibrinous and Organizing Pneumonia Following Hematopoietic Stem Cell Transplantation
- A Case of Parainfluenza Virus Related Acute Respiratory Distress Syndrome in Immune Competent Adult Patient: A Case Report
