Obstructive Fibrinous Tracheal Pseudomenbrane Mimicking Tracheal Stents
- Affiliations
-
- 1Division of Pulmonology, Critical Care Medicine, Department of Internal Medicine, The Catholic University of Korea College of Medicine, Seoul, Korea. ajhcmcim@catholic.ac.kr
Abstract
- Obstructive Fibrinous Tracheal Pseudomenbrane (OFTP) is a rarely known but potentially fatal complication of endotracheal intubation. Sudden respiratory failure shortly after extubation is not infrequent in the ICU. However, these cases are commonly diagnosed as laryngospasm, retention of secretion or laryngeal edema. A 68-year-old woman presented with a 6-day history of progressive dyspnea. She had undergone invasive ventilator care for 24 hours. The patient was discharged from the hospital with improvement after having an extubation. However, after 3 days she revisited the emergency department with progressive dyspnea. The patient was diagnosed with OFTP from the results of chest CT and bronchoscopy. This is the first case studied in detail using CT images, pulmonary function test, and bronchoscopy.
Keyword
MeSH Terms
Figure
-
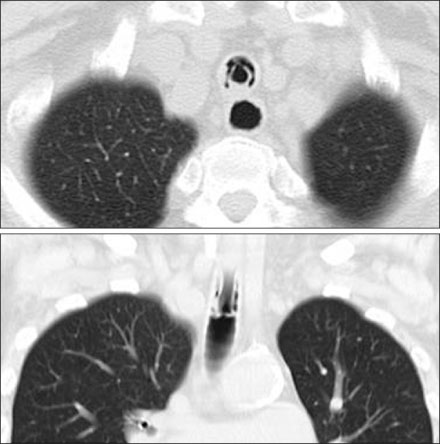
Figure 1 Chest axial and coronal CT images are showing tubular structure with a good patency. It looks like a tracheal stents at upper trachea. CT: computed tomography.
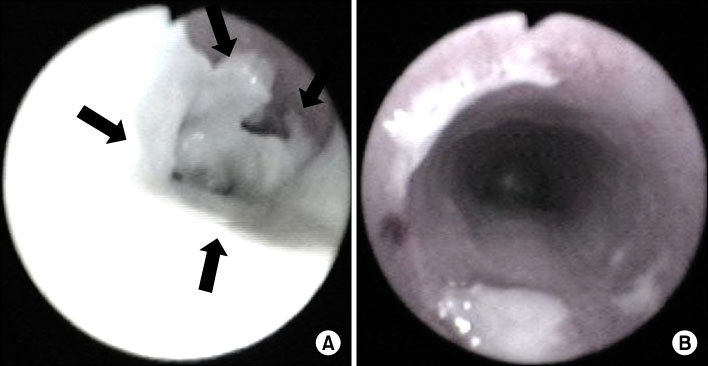
Figure 2 (A) Fiberoptic bronchoscopy showing a thick tubular, rubber-like, whitish pseudomembrane moulding covering 2~3 cm of the tracheal wall at the level of the endotracheal cuff (the arrows indicate the pseudomembrane partially detached from trachea). (B) Fiberoptic bronchoscopy showing good patency after mechanical ablation with fiberoptic bronchoscopy.
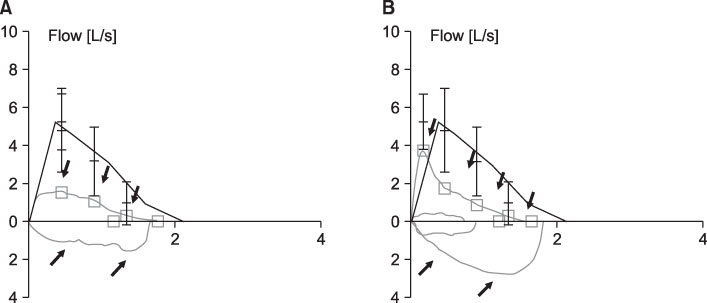
Figure 3 Flow-volume loops showed a fixed airway obstruction before mechanical removal of OFPT (the arrows indicate flow-volume loops) (A) and complete recovery of a fixed airway obstruction after mechanical removal of OFPT (B).
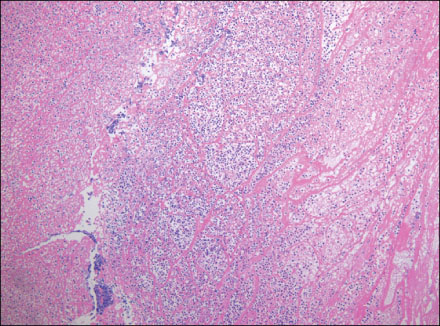
Figure 4 Microscopic examination showing that the pseudomembrane consists of fibrinous material with acute inflammatory cell infiltration (H&E stain, ×100).
Reference
-
1. Deslée G, Brichet A, Lebuffe G, Copin MC, Ramon P, Marquette CH. Obstructive fibrinous tracheal pseudomembrane. A potentially fatal complication of tracheal intubation. Am J Respir Crit Care Med. 2000. 162:1169–1171.2. Lins M, Dobbeleir I, Germonpré P, Waelput W, Pauwels P, Jorens PG. Postextubation obstructive pseudomembranes: a case series and review of a rare complication after endotracheal intubation. Lung. 2011. 189:81–86.3. Harbison J, Collins D, Lynch V, McNicholas WT. Acute stridor due to an upper tracheal membrane following endotracheal intubation. Eur Respir J. 1999. 14:1238.4. Kang HH, Kim JW, Kang JY, Kim JS, Kim MS, Kim SS, et al. Obstructive fibrinous tracheal pseudomembrane after tracheal intubation: a case report. J Korean Med Sci. 2010. 25:1384–1386.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Obstructive Fibrinous Tracheal Pseudomembrane After Tracheal Intubation: A Case Report
- Obstructive Fibrinous Tracheal Pseudomembrane Presented with Atelectasis
- The Safety and efficacy of a new self-expandable intratracheal nitinol stent for the tracheal collapse in dogs
- An Anesthetic Experience of Intratracheal Double-Stents Insertion in an Infant
- Tracheal augmentation with Bovine pericardium
