Prostatic Cancer Presenting as an Isolated Large Lung Mass
- Affiliations
-
- 1Department of Internal Medicine, Korea Cancer Center Hospital, Seoul, Korea. jclee@kcch.re.kr
- 2Department of Pathology, Korea Cancer Center Hospital, Seoul, Korea.
Abstract
- A hidden primary tumor presenting as an isolated lung mass is a diagnostic challenge to physicians because the diagnosis of lung cancer is likely to be made if the histologic findings are not inconsistent with lung cancer. A large lung mass was found incidentally in a 59-year-old man. Although adenocarcinoma was diagnosed by percutaneous needle biopsy, thyroid transcription factor-1 (TTF-1) immunostaining was negative, raising suspicion that there was another primary site. There was no abnormal finding except for the lung mass on a 18FDG-PET/CT scan and the patient did not complain of any discomfort. Finally, prostatic cancer was confirmed through the study of tumor markers and prostate-specific antigen (PSA) immunostaining. Because of the rare presentation of a single lung mass in malignancies that have another primary site, physicians should carefully review all data before making a final diagnosis of lung cancer.
MeSH Terms
Figure
-
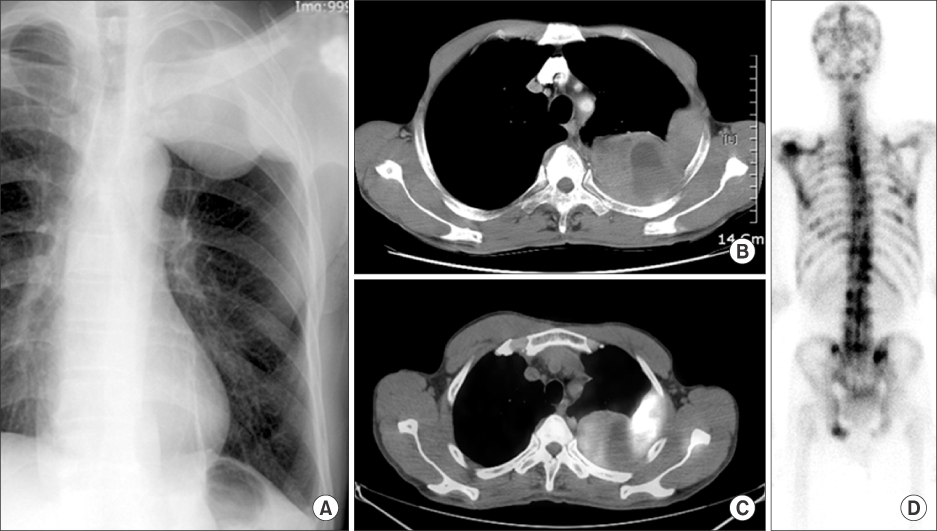
Figure 1 (A) Chest radiograph showed a large lung mass on left upper lung. (B) A lung mass with central necrosis along posterior pleural surface was noted on chest CT. (C) Uneven 18FDG uptake of the lung mass was revealed on PET/CT. (D) Bone scan showed multiple metastatic bony lesions.
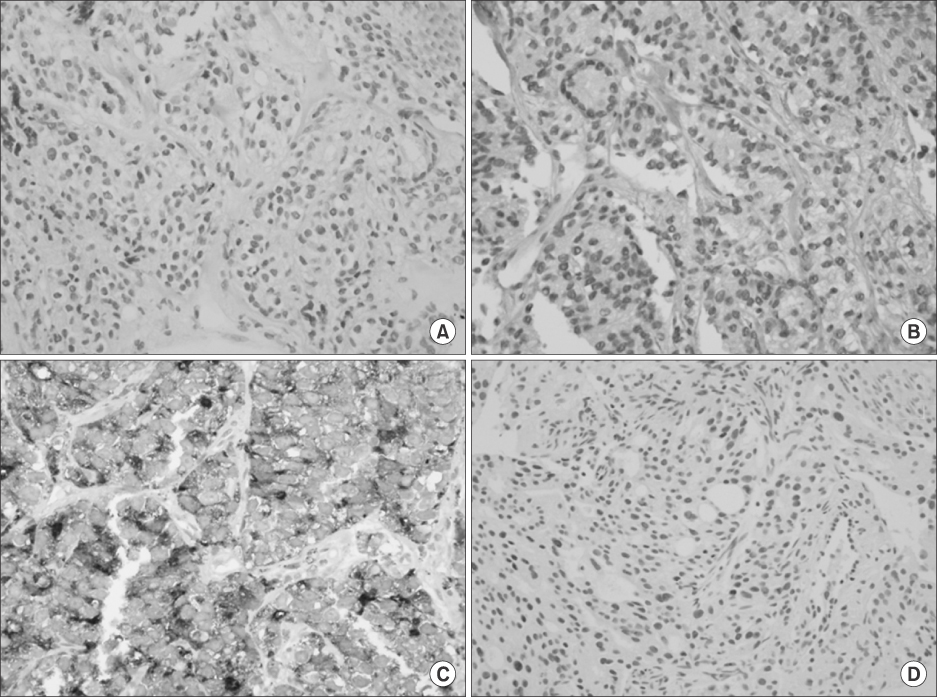
Figure 2 (A) Adenocarcinoma was diagnosed by percutaneous needle biopsy from lung tumor (H&E stain, ×200). (B) TTF-1 immunostaining of lung tumor was negative (TTF-1 immunostain, ×200). (C) PSA immunostaining of lung tumor tissues was strong positive (PSA immunostain, ×400). (D) Prostatic biopsy showed almost same morphologic features with lung tumor (H&E stain, ×200).
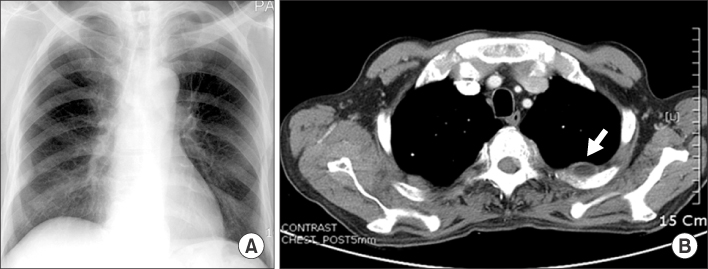
Figure 3 (A) The size of huge lung mass was markedly reduced by treatment with a luteinizing hormone-releasing hormone agonist on chest radiograph. (B) Chest CT also showed the shrunken mass with necrosis (arrow).
Reference
-
1. Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007. 57:43–66.2. Sim HG, Cheng CW. Changing demography of prostate cancer in Asia. Eur J Cancer. 2005. 41:834–845.3. Bubendorf L, Schöpfer A, Wagner U, Sauter G, Moch H, Willi N, et al. Metastatic patterns of prostate cancer: an autopsy study of 1,589 patients. Hum Pathol. 2000. 31:578–583.4. Fabozzi SJ, Schellhammer PF, el-Mahdi AM. Pulmonary metastases from prostate cancer. Cancer. 1995. 75:2706–2709.5. Zelefsky MJ, Eastham JA, Sartor OA, Kantoff P. Devita VT, Lawrence TS, Rosenberg S, editors. Chapter 40. Cancers of the genitourinary system. Cancer: principles and practice of oncology. 2008. 8th ed. Philadelphia: Lippincott Williams & Wilkins;1392–1462.6. Travis WD, Travis LB, Devesa SS. Lung cancer. Cancer. 1995. 75:191–202.7. Devesa SS, Bray F, Vizcaino AP, Parkin DM. International lung cancer trends by histologic type: male:female differences diminishing and adenocarcinoma rates rising. Int J Cancer. 2005. 117:294–299.8. Yamada T, Ono S, Tsuboi M, Saito H, Sato A, Matsuhashi T, et al. Low-dose CT of the thorax in cancer follow-up. Eur J Radiol. 2004. 51:169–174.9. Weng MJ, Wu MT, Pan HB, Kan YY, Yang CF. The feasibility of low-dose CT for pulmonary metastasis in patients with primary gynecologic malignancy. Clin Imaging. 2004. 28:408–414.10. King JE, Thatcher N, Pickering CA, Hasleton PS. Sensitivity and specificity of immunohistochemical markers used in the diagnosis of epithelioid mesothelioma: a detailed systematic analysis using published data. Histopathology. 2006. 48:223–232.11. Choi YH, Park KY, Ryoo BY, Na II, Yang SH, Koh JS, et al. Presence of malignant mesothelial cells in the sputum. Intern Med. 2008. 47:57–60.12. Moldvay J, Jackel M, Bogos K, Soltész I, Agócs L, Kovács G, et al. The role of TTF-1 in differentiating primary and metastatic lung adenocarcinomas. Pathol Oncol Res. 2004. 10:85–88.13. Abutaily AS, Addis BJ, Roche WR. Immunohistochemistry in the distinction between malignant mesothelioma and pulmonary adenocarcinoma: a critical evaluation of new antibodies. J Clin Pathol. 2002. 55:662–668.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cutaneous Metastasis from Prostatic Cancer
- Computer-aided Diagnosis for Lung Cancer
- Solitary Pulmonary Metastasis of a Thyroid Papillary Microcarcinoma, Masquerading as Primary Lung Cancer
- Nodular scalp mass as the first presentation of pulmonary large cell neuroendocrine carcinoma: a case report
- Small Cell Lung Cancer at Subcarina Presenting as a Metastatic Brain Tumor
