Solitary Pulmonary Metastasis of a Thyroid Papillary Microcarcinoma, Masquerading as Primary Lung Cancer
- Affiliations
-
- 1Department of Internal Medicine, Korea Cancer Center Hospital, Seoul, Korea. jclee@amc.seoul.kr
- 2Department of Pathology, Korea Cancer Center Hospital, Seoul, Korea.
- KMID: 2169129
- DOI: http://doi.org/10.3803/EnM.2011.26.1.78
Abstract
- Although pulmonary metastasis of thyroid cancer is not uncommon, it mostly occurs as multiple discrete nodules on the lung parenchyma. Because thyroid cancer presenting with an isolated large lung mass is extremely rare and the diagnosis is frequently based on small pieces of tissue obtained by a fine needle, the wrong diagnosis such as lung cancer is prone to be made. A 60-year-old man was admitted for evaluation of a lung mass detected on chest radiography. Cytological examination of the bronchial washing specimens suggested adenocarcinoma. Surgery for early lung cancer was performed considering that no other abnormalities were found during the work-up that included 18-fludeoxyglucose positron emission tomography computer tomography (18FDG-PET/CT). Unexpectedly, the diagnosis of papillary thyroid cancer with lung metastasis was made, which prompted us to evaluate the thyroid gland and then remove the primary cancer by subsequent operation. Although it is uncommon, physician should be aware of this possibility, which could help to avoid the wrong diagnosis. Here we report on a typical case of solitary pulmonary metastasis of thyroid cancer and we summarize the previously reported cases with a review of the relevant literature.
Keyword
MeSH Terms
Figure
-

Fig. 1 Simple chest X-ray, CT and 18FDG-PET/CT findings. A. Chest radiograph showed a round mass behind cardiac shadow in left lower lobe (arrow). B. An about 2.9 cm-sized mass in the central portion of left lower lobe was found on chest CT. C. 18FDG-PET/CT revealed a hypermetabolic lesion with SUV of 4.5.
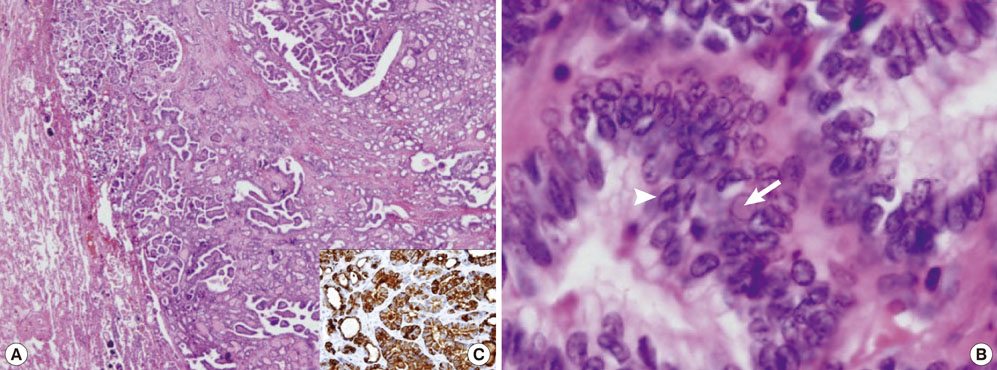
Fig. 2 Pathologic findings. A, B. Pathologic examination of the resected lung tumor showed typical tumor cells of papillary thyroid carcinoma (H&E staining; A, × 40) with nuclear groove (arrowhead) and intranuclear inclusions (arrow) (H&E staining; B, × 400). C. The immunohistological staining for thyroglobulin was strong-positive.
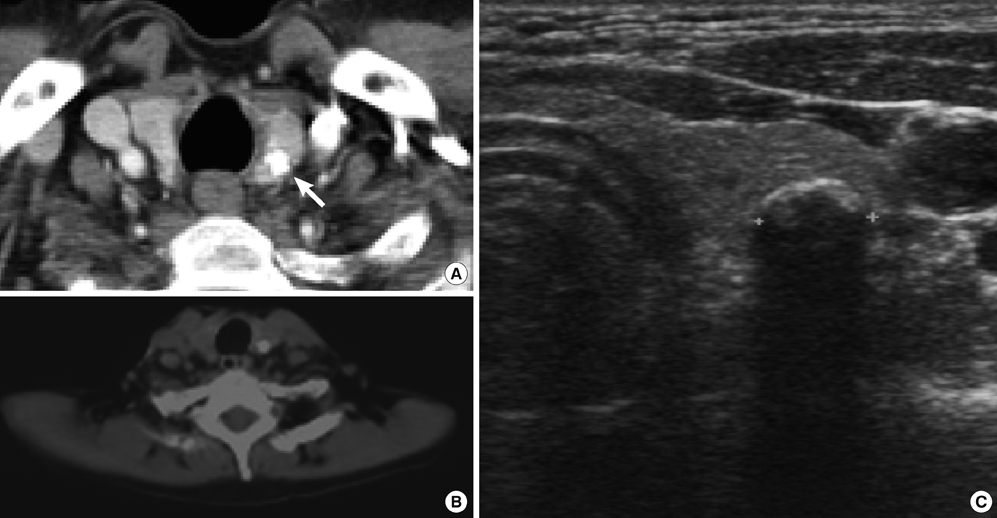
Fig. 3 Neck CT, 18FDG-PET/CT and ultrasound findings. A. 0.6 cm calcified nodule in left thyroid gland (arrow) and multiple small cysts and nodular hyperplasia in both thyroid glands were noted. B. There was no definite FDG uptake around the calcified nodule. C. An about 0.6 cm dense, round calcified nodule with posterior shadowing in left thyroid gland (arrow) and was found on thyroid ultrasonogram.
Reference
-
1. Henschke CI, McCauley DI, Yankelevitz DF, Naidich DP, McGuinness G, Miettinen OS, Libby DM, Pasmantier MW, Koizumi J, Altorki NK, Smith JP. Early Lung Cancer Action Project: overall design and findings from baseline screening. Lancet. 1999. 354:99–105.2. Kim YK, Chung JK, Kim SK, Yeo JS, Park DJ, Jeong JM, Lee DS, Cho BY, Lee MC. Results of radioiodine treatment for distant metastases of differentiated thyroid carcinoma. Korean J Nucl Med. 2000. 34:107–118.3. Trinidad S, Lisa JR, Rosenblatt MB. Bronchogenic Carcinoma Simulated by Metastatic Tumors. Cancer. 1963. 16:1521–1529.4. Cahan WG, Shah JP, Castro EB. Benign solitary lung lesions in patients with cancer. Ann Surg. 1978. 187:241–244.5. Snyder BJ, Pugatch RD. Imaging characteristics of metastatic disease to the chest. Chest Surg Clin N Am. 1998. 8:29–48.6. Coppage L, Shaw C, Curtis AM. Metastatic disease to the chest in patients with extrathoracic malignancy. J Thorac Imaging. 1987. 2:24–37.7. Wada N, Duh QY, Sugino K, Iwasaki H, Kameyama K, Mimura T, Ito K, Takami H, Takanashi Y. Lymph node metastasis from 259 papillary thyroid microcarcinomas: frequency, pattern of occurrence and recurrence, and optimal strategy for neck dissection. Ann Surg. 2003. 237:399–407.8. Schlumberger MJ. Papillary and follicular thyroid carcinoma. N Engl J Med. 1998. 338:297–306.9. Schlumberger M, Tubiana M, De Vathaire F, Hill C, Gardet P, Travagli JP, Fragu P, Lumbroso J, Caillou B, Parmentier C. Long-term results of treatment of 283 patients with lung and bone metastases from differentiated thyroid carcinoma. J Clin Endocrinol Metab. 1986. 63:960–967.10. Mazzaferri EL. An overview of the management of papillary and follicular thyroid carcinoma. Thyroid. 1999. 9:421–427.11. Zettinig G, Fueger BJ, Passler C, Kaserer K, Pirich C, Dudczak R, Niederle B. Long-term follow-up of patients with bone metastases from differentiated thyroid carcinoma -- surgery or conventional therapy? Clin Endocrinol (Oxf). 2002. 56:377–382.12. Wood WJ Jr, Singletary SE, Hickey RC. Current results of treatment for distant metastatic well-differentiated thyroid carcinoma. Arch Surg. 1989. 124:1374–1377.13. Casara D, Rubello D, Saladini G, Masarotto G, Favero A, Girelli ME, Busnardo B. Different features of pulmonary metastases in differentiated thyroid cancer: natural history and multivariate statistical analysis of prognostic variables. J Nucl Med. 1993. 34:1626–1631.14. Schlumberger M, Challeton C, De Vathaire F, Travagli JP, Gardet P, Lumbroso JD, Francese C, Fontaine F, Ricard M, Parmentier C. Radioactive iodine treatment and external radiotherapy for lung and bone metastases from thyroid carcinoma. J Nucl Med. 1996. 37:598–605.15. Hay ID, Grant CS, van Heerden JA, Goellner JR, Ebersold JR, Bergstralh EJ. Papillary thyroid microcarcinoma: a study of 535 cases observed in a 50-year period. Surgery. 1992. 112:1139–1146. discussion 1146-1137.16. Pellegriti G, Scollo C, Lumera G, Regalbuto C, Vigneri R, Belfiore A. Clinical behavior and outcome of papillary thyroid cancers smaller than 1.5 cm in diameter: study of 299 cases. J Clin Endocrinol Metab. 2004. 89:3713–3720.17. Sakairi Y, Yasufuku K, Iyoda A, Suzuki M, Nakajima T, Sekine Y, Shibuya K, Takahashi Y, Nakatani Y, Fujisawa T. A solitary metastatic lung tumor from thyroid papillary carcinoma diagnosed by endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA): report of a case. Surg Today. 2008. 38:46–48.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Cystic Lymph Node Metastasis from Thyroid Papillary Microcarcinoma
- Two Cases of Non-Small Cell Lung Cancer Masquerading as Metastatic Papillary Thyroid Cancer
- A Case of Ectopic Thyroid Papillary Carcinoma with Incidental Papillary Thyroid Microcarcinoma
- Metastatic Lung Nodule of Thyroid Papillary Carcinoma, Mimicking Primary Lung Cancer
- Solitary Papillary Thyroid Microcarcinoma (0.3 cm in Diameter) Presenting Multiple Distant Metastases at the Time of Diagnosis
