Two Cases of Non-Small Cell Lung Cancer Masquerading as Metastatic Papillary Thyroid Cancer
- Affiliations
-
- 1Department of Internal Medicine, Chungnam National University College of Medicine, Daejeon, Korea.
- 2Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea. yjparkmd@snu.ac.kr
- 3Department of Pathology Seoul National University College of Medicine, Seoul, Korea.
- 4Department of Radiology, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2095106
- DOI: http://doi.org/10.11106/jkta.2012.5.2.157
Abstract
- Papillary thyroid carcinoma and primary lung cancer have vastly different treatment approaches and prognosis. If lung mass is found in patients with papillary thyroid carcinoma, we have to be aware of the possibility of primary lung cancer especially when the lesion is not iodine-avid, or is not typical to metastatic thyroid carcinoma, or serum thyroglobulin is not elevated. Here we present two cases of non-small cell lung cancer masquerading as metastatic papillary thyroid carcinoma and think of the approach of the lung mass which is found in patients with papillary thyroid carcinoma.
MeSH Terms
Figure
-
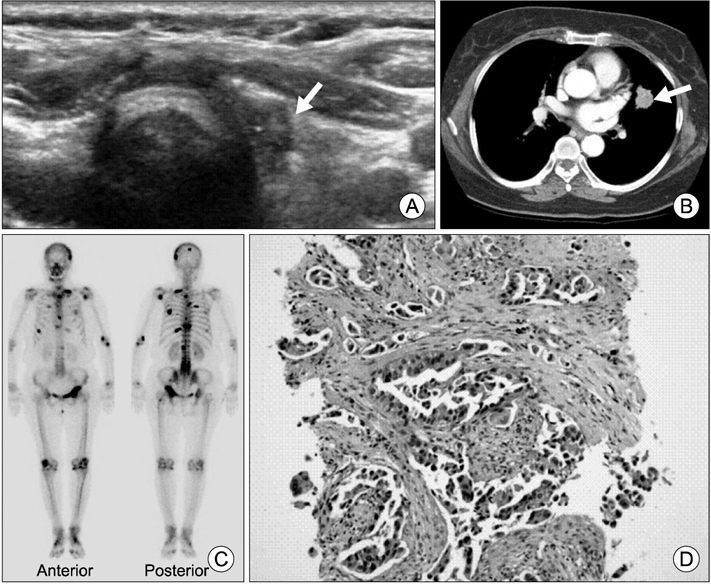
Fig. 1 (A) 0.9 cm sized hypoechoic nodule at the operation bed (arrow) was found on neck ultrasonogram. (B) Chest CT showed 2.4 cm sized nodule (arrow) in left upper lobe lingular division. (C) Bone scan revealed multiple increased uptake in skull, T-L spines, both ribs, left scapula, left humerus, left radius, left pelvic bone and left femur. (D) The lung biopsy was diagnosed as primary well-differentiated adenocarcinoma (H&E stain, ×200).
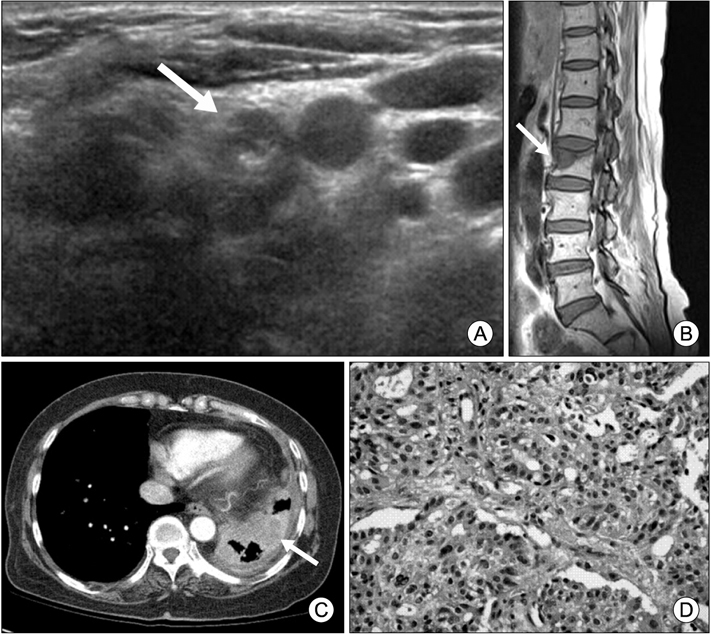
Fig. 2 (A) Neck ultrasonography showed metastatic lymph nodes (arrow) in left neck level VI. (B) L-spine MRI showed L2 compression fracture (arrow). (C) Chest CT showed diffuse irregular pleural thickening with pleural masses (arrow) in left hemithorax. (D) The lung needle biopsy was non small cell carcinoma focally showing gland-forming features, which was suggestive of adenocarcinoma of lung (H&E stain, ×400).
Reference
-
1. The Korea Central Cancer Registry. National Cancer Center. Annual report of cancer statistics in Korea in 2008. 2010. Seoul, Korea: Ministry of Health and Welfare.2. Lee YJ, Han JY. Current trends in early diagnosis and treatment of lung cancer. Korean J Med. 2011. 80(5):529–531.3. Sipos JA, Mazzaferri EL. Thyroid cancer epidemiology and prognostic variables. Clin Oncol (R Coll Radiol). 2010. 22(6):395–404.
Article4. Sampson E, Brierley JD, Le LW, Rotstein L, Tsang RW. Clinical management and outcome of papillary and follicular (differentiated) thyroid cancer presenting with distant metastasis at diagnosis. Cancer. 2007. 110(7):1451–1456.
Article5. Lee J, Soh EY. Differentiated thyroid carcinoma presenting with distant metastasis at initial diagnosis clinical outcomes and prognostic factors. Ann Surg. 2010. 251(1):114–119.
Article6. Yi KH, Park YJ, Koong SS, Kim JH, Na DG, Ryu JS, et al. Revised Korean Thyroid Association management guidelines for patients with thyroid nodules and thyroid cancer. Endocrinol Metab. 2010. 25(4):270–297.
Article7. Lind P, Kohlfurst S. Respective roles of thyroglobulin, radioiodine imaging, and positron emission tomography in the assessment of thyroid cancer. Semin Nucl Med. 2006. 36(3):194–205.
Article8. Lin JD, Chao TC, Chou SC, Hsueh C. Papillary thyroid carcinomas with lung metastases. Thyroid. 2004. 14(12):1091–1096.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- An Unusual Case of Metastatic Non-Small Cell Lung Cancer Misidentified as Anaplastic Thyroid Cancer
- Effect of Afatinib for Lung Cancer on Papillary Thyroid Carcinoma
- Systemic Sclerosis Associated with Non-small Cell Lung Cancer and Papillary Thyroid Cancer: Case Report and Literature Review
- Metastatic Lung Nodule of Thyroid Papillary Carcinoma, Mimicking Primary Lung Cancer
- Concurrent Primary Carcinoma and Metastatic Lesions of the Thyroid
