Relationship between Pleural Adenosine Deaminase Level and Patterns of Pleural Enhancement in Patients with a Tuberculous Pleural Effusion on CT Scan
- Affiliations
-
- 1Department of Diagnostic Radiology, Hospital of Chung Ang University, Seoul, Korea. hynlee1@hanmail.net
Abstract
- Background
This study examined the relationship between the pleural adenosine deaminase (ADA) level and the patterns of pleural enhancement in patients with a tuberculous pleural effusion (TPE) shown on a CT scan. Methods: The charts and CT findings of 44 patients with TPE from February 2002 to October 2006 were reviesed retrospectively. A diagnosis of TPE was made by the pleural ADA level with a follow-up (24/44), sputum smear or culture of sputum (16/44), pleural fluid culture (3/44) or pleural biopsy (1/44). The patients were divided into two groups according to the ADA level(Group I [n=12]: 40-70, Group II [n=32]: >70 U/L). The presence or absence, maximal thickness and patterns of pleural enhancement were analyzed. The pattern of pleural enhancement was classified into diffuse or focal, smooth or irregular and interrupted or continuous. The difference in CT findings between groups I and group II were analyzed using an unpaired T test, Chi-square test and Z test. Results: All 44 patients showed diffuse pleural enhancement on the CT scans. The maximal pleural thickness of groups I and II was 1.83 +/- 1.03 mm (1-4 mm) and 3.63 +/- 1.78 mm (1-8 mm), respectively (p =0.0002). Pleural thickening > or = 5 mm was only demonstrated in 31.3% of patients in group II (10/32). Diffuse interrupted pleural thickening was noted in 91.7% (11/12) of patients in group I and 62.5% (20/32) in group II, respectively. Diffuse continuous pleural thickening was observed in 8.3% (1/12) of patients in group I and 37.5% (12/32) in group II, respectively (p=0.0748). Conclusion: Pleural thickening > or = 5 mm on the contrast enhanced CT is rare in patients with lymphocyte-dominant TPE in whom the pleural ADA level is between 40-70 U/L.
Keyword
MeSH Terms
Figure
-

Figure 1 Diffuse, intermittent, and smooth pleural enhancement pattern in a 58-year-old man with a tuberculous pleural effusion on the contrast-enhanced CT scan (ADA level, 46 U/L). Diffuse, intermittent, and smooth pleural enhancement (arrows) with a right pleural effusion is noted at the level of the left atrium on a contrast-enhanced CT scan. The maximal thickness of pleural enhancement is approximately 2 mm.
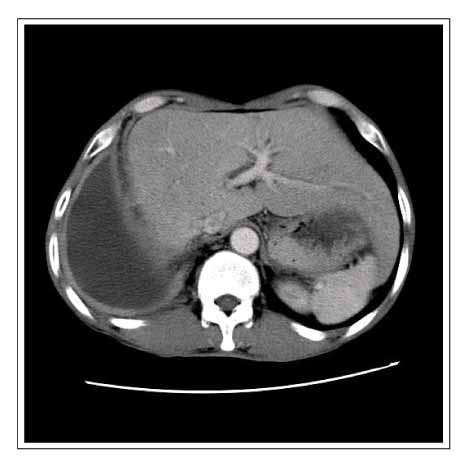
Figure 2 Diffuse, continuous, and smooth pleural enhancement pattern in a 28-year-old man with tuberculous pleural effusion on the contrast-enhanced CT scan (ADA level, 120 U/L). Diffuse, continuous, and smooth pleural enhancement (arrows) with a right pleural effusion is noted at the level of the liver on the contrast-enhanced CT scan. The maximal thickness of pleural enhancement is about 6 mm.
Reference
-
1. Roth BJ. Searching for tuberculosis in the pleural space. Chest. 1999. 116:3–5.2. Riantawan P, Chaowalit P, Wongsangiem M, Rojanaraweewong P. Diagnostic value of pleural fluid adenosine deaminase in tuberculous pleuritis with reference to HIV coinfection and a Bayesian analysis. Chest. 1999. 116:97–103.3. Valdes L, Alvarez D, San Jose E, Penela P, Valle JM, Garcia-Pazos JM, et al. Tuberculous pleurisy: a study of 254 patients. Arch Intern Med. 1998. 158:2017–2021.4. Valdes L, San Jose E, Alvarez D, Valle JM. Adenosine deaminase (ADA) isoenzyme analysis in pleural effusions: diagnostic role, and relevance to the origin of increased ADA in tuberculous pleurisy. Eur Respir J. 1996. 9:747–751.5. Burgess LJ, Maritz FJ, Le Roux I, Taljaard JJ. Combined use of pleural adenosine deaminase with lymphocyte/neutrophil ratio. Increased specificity for the diagnosis of tuberculous pleuritis. Chest. 1996. 109:414–419.6. Laniado-Laborin R. Adenosine deaminase in the diagnosis of tuberculous pleural effusion: is it really an ideal test? A word of caution. Chest. 2005. 127:417–418.7. Moon JW, Han CH, Kang SM, Park MS, Hwang SY, Byun MK, et al. The relationship between age and pleural fluid adenosine deaminase activity in pleural tuberculosis. Tuberc Respir Dis. 2005. 58:459–464.8. Giusti G. Bergmeyer HU, editor. Adenosine deaminase. Methods of enzymate analysis. 1974. New York, NY: Academic Press;1092–1099.9. Antony VB. Adenosine deaminase isoenzymes and pleural tuberculosis. J Lab Clin Med. 1996. 127:326–327.10. Lee YC, Rogers JT, Rodriguez RM, Miller KD, Light RW. Adenosine deaminase levels in nontuberculous lymphocytic pleural effusions. Chest. 2001. 120:356–361.11. Shibagaki T, Hasegawa Y, Saito H, Yamori S, Shimokata K. Adenosine deaminase isozymes in tuberculous pleural effusion. J Lab Clin Med. 1996. 127:348–352.12. Aoki Y, Katoh O, Nakanishi Y, Kuroki S, Yamada H. A comparison study of IFN-gamma, ADA, and CA125 as the diagnostic parameters in tuberculous pleuritis. Respir Med. 1994. 88:139–143.13. Fontan Bueso J, Verea Hernando H, Garcia-Buela JP, Dominguez Juncal L, Martin Egana MT, Montero Martinez MC. Diagnostic value of simultaneous determination of pleural adenosine deaminase and pleural lysozyme/serum lysozyme ratio in pleural effusions. Chest. 1988. 93:303–307.14. Valdes L, San Jose E, Alvarez D, Sarandeses A, Pose A, Chomon B, et al. Diagnosis of tuberculous pleurisy using the biologic parameters adenosine deaminase, lysozyme, and interferon gamma. Chest. 1993. 103:458–465.15. Light RW. Pleural disease. 2001. 4th ed. Baltimore, MD: Williams & Wilkins.16. Ocana I, Martinez-Vazquez JM, Segura RM, Fernandez-De-Sevilla T, Capdevila JA. Adenosine deaminase in pleural fluids: test for diagnosis of tuberculous pleural effusion. Chest. 1983. 84:51–53.17. Damas P, Canivet JL, de Groote D, Vrindts Y, Albert A, Franchimont P, et al. Sepsis and serum cytokine concentrations. Crit Care Med. 1997. 25:405–412.18. Ertel W, Morrison MH, Wang P, Ba ZF, Ayala A, Chaudry IH. The complex pattern of cytokines in sepsis. Association between prostaglandins, cachectin, and interleukins. Ann Surg. 1991. 214:141–148.19. Johns DG, Webb RC. TNF-alpha-induced endothelium-independent vasodilation: a role for phospholipase A2-dependent ceramide signaling. Am J Physiol. 1998. 275:1592–1598.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Utility of Pleural Adenosine Deaminase for Diagnosis of Differentiating Tuberculous Pleural Effusion in Children
- Diagnostic Efficacy of Adenosine Deaminase Isoenzyme in Tuberculous Pleurisy
- Relationship Between Age and Pleural Fluid Adenosine Deaminase Activity in Patients with Tuberculous Pleural Effusion
- Diagnostic Value of Adenosine Deaminase(ADA) and its Isoenzyme in Pleural Effusion
- Tuberculous Pleurisy: An Update
