Teratoma Presenting as An Unilateral Mediastinal Mass with Contralateral Pleural Effusion
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Korea University, Seoul, Korea. chepraxis@korea.com
- 2Department of Thoracic and Cardiovascular Surgery, College of Medicine, Korea University, Seoul, Korea.
- 3Department of Pathology, College of Medicine, Korea University, Seoul, Korea.
Abstract
- A teratoma is the most common benign germ cell tumor that develops in the mediastinum. Patients with a mediastinal teratoma are usually asymptomatic. However, a spontaneous rupture of a mediastinal teratoma into the pleural cavity or adjacent organs can cause severe chest pain, hemoptysis, acute dyspnea, etc. Complications such as recurrent pneumonia, pericardial effusion, pleural effusion and great vessel invasion can sometimes occur. We encountered a case of a patient with an abrupt onset of dyspnea after persistent shoulder pain for one month. The X-ray examinations revealed a unilateral mediastinal mass with contralateral pleural effusion. Subsequent evaluations confirmed a spontaneous rupture of the teratoma into the contralateral pleural cavity.
MeSH Terms
Figure
-
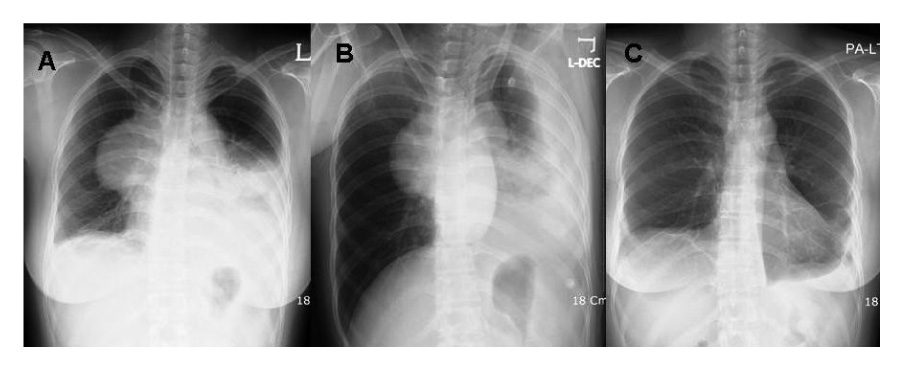
Figure 1 Chest radiography shows a huge mass lesion in right hilar area (A), blunting of left costophrenic angle with fluid shifting (B) on admission, and near-normal findings 2 months later after surgical resection (C).

Figure 2 Chest computed tomography shows a 6×7 cm sized, septated cystic mass, containing a fat-like low density component in the anterior mediastinum, which insinuates between superior vena cava and ascending aorta (A). The wall of mass is enhanced and no calcification is visible. Left pleural effusion and passive atelectasis are also noted (B).

Figure 3 Intraoperative photographs of excised specimen (A, B) showed several fragments of yellow to brown soft tissue, measuring 4.7×3×3 cm in the largest one. The histologic findings of specimens are consistent with ruptured teratoma, and reveal adipose tissue (C), formation of pancreatic acini and islet-like stucture (D). (hematoxylin and eosin, C:×100, D:×200)
Reference
-
1. Cancer principles & practice of oncology. 2001. 6th ed. Wilkins & Wilkins.2. Moeller KH, Rosado-de-Christenson ML, Templeton PA. Mediastinal mature teratoma: imaging features. AJR Am J Roentgenol. 1997. 169:985–990.3. Gunes S, Varon J, Walsh G. Mediastinal teratoma presenting as massive hemoptysis in an adult. J Emerg Med. 1997. 15:313–316.4. Oomman A, Santhosham R, Vijayakumar C, Jayaraman S, Ramachandran P, Kumar S. Anterior mediastinal teratoma presenting as cardiac tamponade. Indian Heart J. 2004. 56:64–66.5. Sasaka K, Kurihara Y, Nakajima Y, Seto Y, Endo I, Ishikawa T, et al. Spontaneous rupture: a complication of benign mature teratomas of the mediastinum. AJR Am J Roentgenol. 1998. 170:323–328.6. Cheung YC, Ng SH, Wan YL, Pan KT. Ruptured mediastinal cystic teratoma with intrapulmonary bronchial invasion: CT demonstration. Br J Radiol. 2001. 74:1148–1149.7. Ozergin U, Gormus N, Aribas OK, Durgut K, Yuksek T. Benign mature cystic teratoma of the anterior mediastinum leading to heart failure: report of a case. Surg Today. 2003. 33:518–520.8. Pack HM, Kim ES, Kang JH, Jee HO. Anterior mediastinal teratoma which complicated empyema. Korean J Thorac Cardiovasc Surg. 1988. 21:535–540.9. Lee TH, Lee SE, Baik JJ, Chung Y. A case of mediastinal teratoma complicated by spontaneous ruptured into pleural cavity. Tuberc Respir Dis. 1999. 47:265–271.10. Jeon JB, Chung CH, Moon TH, Cho W, Ryu JS, Kwak SM, et al. Spontaneuos rupture of mediastinal teratoma into adjacent tissue. Tuberc Respir Dis. 1999. 47:400–405.11. Choi SJ, Lee JS, Song KS, Lim TH. Mediastinal teratoma: CT differentiation of ruptured and unruptured tumors. AJR Am J Roentgenol. 1998. 171:591–594.12. Goldstraw P. Spontaneous intrapleural rupture of mediastinal teratoma. Respir Med. 1993. 87:399–400.13. Ege G, Akman H, Cakiroglu G, Kalayci G. Spontaneous rupture of mediastinal cystic teratoma with high levels of amylase, lipase, CA 19-9, CA 125 and CEA in cystic fluid: a case report. Acta Radiol. 2004. 45:111–112.14. Kimura C, Kamiyoshihara M, Sakata K, Itoh H, Morishita Y. Mediastinal mature teratoma perforating Into the lung with elevated serum carbohydrate antigen 19-9 (CA19-9) levels: report of a case. Kyobu Geka. 2003. 56:247–250.15. Cho JH, Son HS, Jo WM, Min BJ, Lee IS, Shin JS. Treatment of mediastinal growing teratoma syndrome. Korean J Thorac Cardiovasc Surg. 2005. 38:729–732.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Medistinal Teratoma with Pleural and Pericardial Effusion Teratoma with Pleural and Pericardial Effusion
- A Case of Mediastinal Teratoma Complicated by Spontaneous Rupture into Pleural Cavity
- Rupture of Mediastinal Mature Teratoma into the Pleural Cavity: A Case Report
- A Case of Thymic Mature Teratoma with Massive Pleural Effusion
- Spontaneous Rupture of Mediastinal Teratoma into Adjacent Tissues
