A Case of Constrictive Pericarditis due to Immunoglobulin G4-Related Disease
- Affiliations
-
- 1Division of Cardiology, Yonsei University College of Medicine, Seoul, Korea. shpark0530@yuhs.ac
- 2Department of Thoracic and Cardiovascular Surgery, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea.
- 3Department of Pathology, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2297884
- DOI: http://doi.org/10.4070/kcj.2015.45.2.161
Abstract
- Immunoglobulin G4-related disease (IgG4-RD) can involve any organ. The majority of reported cases involve IgG4-RD of the biliary tract or pancreas, while only two cases of pericarditis have been reported. A 58-year-old man visited the outpatient clinic of our institution with a seven-day history of progressive dyspnea. Based on his transthoracic echocardiogram and transesophageal echocardiogram, he was diagnosed with constrictive pericarditis. The histopathology of his pericardiectomy revealed the cause of constrictive pericarditis to be IgG4-RD. Prednisolone (40 mg) was initiated after the pericardiectomy. As the patient's symptoms resolved, he was discharged and followed-up on an outpatient basis. This is the first case report of constrictive pericarditis caused by IgG4-RD in Korea.
MeSH Terms
Figure
-

Fig. 1 Chest X-ray on the first day of hospitalization and 8 days after pericardiectomy. A: bilateral pleural effusion with loculation along the right minor fissure with moderate cardiomegaly. B: regression of bilateral plerual effusion and cardiomegaly were detected.
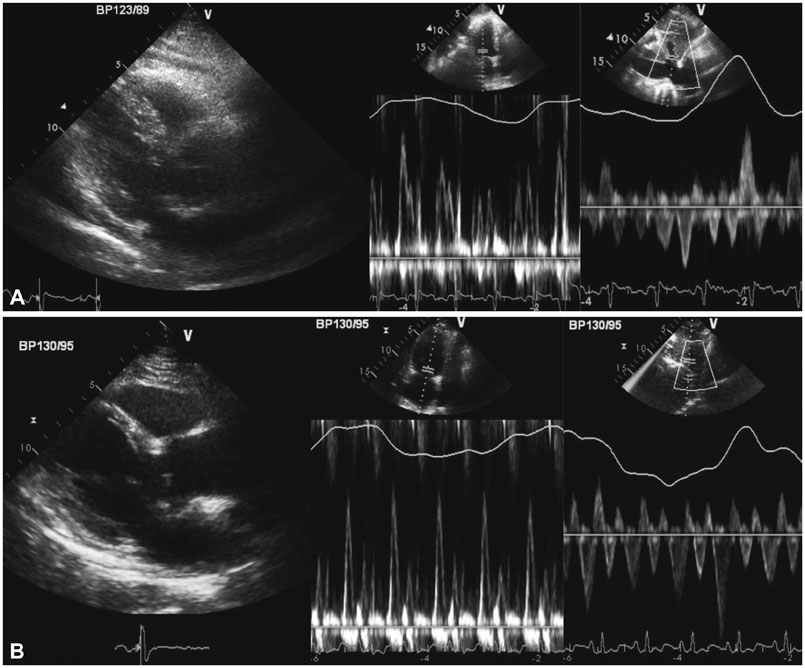
Fig. 2 A: constrictive physiology was observed on the transthoracic echocardiogram on the first day of hospitalization. Septal bouncing motion, respiratory variation of the mitral valve E velocity (55%), expiratory diastolic flow reversal of hepatic vein, and inferior vena cava plethora (29 mm) were observed. B: improved septal bouncing motion, respiratory variation of mitral valve E velocity, and inferior vena cava plethora (24 mm) were observed on the transthoracic echocardiogram 6 months after the pericardiectomy.
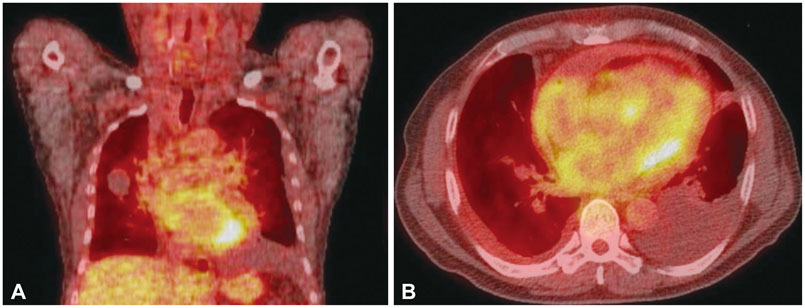
Fig. 3 Positron emission tomography-computed tomography images, coronal (A) and axial (B) section. Pericardial effusion with mild fluorodeoxyglucose-uptake, likely due to inflammatory processes, was observed but there was no evidence of pulmonary tuberculosis
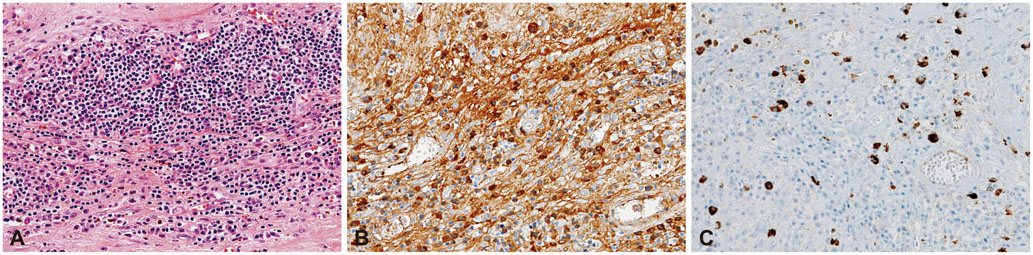
Fig. 4 Histopathological appearance of pericardium. A: hematoxylin-eosin (H&E) stained section of the pericardium revealed a dense lymphoplasmacytic infiltration, sclerosis, and diffuse coating of fibrinous exudate (×200). B: immunostaining for IgG demonstrated numerous IgG-positive plasma cells, with some forming aggregates (×200). C: immunostaining for IgG4 demonstrated an increased absolute count of IgG4-positive cells (30 per high power field on average, counted from 5 hot spots), and the ratio of IgG4/IgG positive cells was 5% (×200). IgG4: immunoglobulin G4.
Reference
-
1. Deshpande V, Zen Y, Chan JK, et al. Consensus statement on the pathology of IgG4-related disease. Mod Pathol. 2012; 25:1181–1192.2. Khosroshahi A, Stone JH. A clinical overview of IgG4-related systemic disease. Curr Opin Rheumatol. 2011; 23:57–66.3. Kamisawa T, Okamoto A, Funata N. Clinicopathological features of autoimmune pancreatitis in relation to elevation of serum IgG4. Pancreas. 2005; 31:28–31.4. Khosroshahi A, Stone JH. Treatment approaches to IgG4-related systemic disease. Curr Opin Rheumatol. 2011; 23:67–71.5. Cheuk W, Chan JK. IgG4-related sclerosing disease: a critical appraisal of an evolving clinicopathologic entity. Adv Anat Pathol. 2010; 17:303–332.6. Imazio M, Brucato A, Maestroni S, et al. Risk of constrictive pericarditis after acute pericarditis. Circulation. 2011; 124:1270–1275.7. Spodick DH. Etiologic spectrum of constrictive pericarditis. Am Heart J. 1987; 114:1529–1530.8. Sekiguchi H, Horie R, Suri RM, Yi ES, Ryu JH. Constrictive pericarditis caused by immunoglobulin G4-related disease. Circ Heart Fail. 2012; 5:e30–e31.9. Sekiguchi H, Horie R, Utz JP, Ryu JH. IgG4-related systemic disease presenting with lung entrapment and constrictive pericarditis. Chest. 2012; 142:781–783.10. Reuter H, Burgess L, van Vuuren W, Doubell A. Diagnosing tuberculous pericarditis. QJM. 2006; 99:827–839.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Constrictive Pericarditis with Localized Pericardial Effusion Simulating a Cystic Mass
- Constrictive Pericarditis Following Acute Idiopathic Pericarditis
- Tuberculous Constrictive Pericarditis: A Classical Case and Review
- A Case of Effusive-Constrictive Pericarditis in and Infant Treated by Pericardiectomy
- Constrictive Pericarditis as a Never Ending Story: What's New?
