J Gynecol Oncol.
2011 Jun;22(2):97-102. 10.3802/jgo.2011.22.2.97.
Major surgeries performed for gestational trophoblastic neoplasms in a teaching hospital in Tehran, Iran
- Affiliations
-
- 1Gynecology Oncology, Tehran University of Medical Sciences, Tehran, Iran.
- 2Gynecology Oncology, Gynecology Department, Afzalipoor Hospital, Kerman University of Medical Sciences, Kerman, Iran. dr_ganjooei@hotmail.com
- KMID: 2288573
- DOI: http://doi.org/10.3802/jgo.2011.22.2.97
Abstract
OBJECTIVE
This study aim was to evaluate indications and outcomes of surgical interventions performed in patients with gestational trophoblastic neoplasm.
METHODS
During January 1995 to December 2005, 110 patients with a diagnosis of persistent gestational trophoblastic neoplasm were treated in our Gynecologic Oncologic Department. Risk score calculation was carried out based on the revised FIGO 2000 scoring system for gestational trophoblastic neoplasm. Data from the patients' records and pathologic reports were analyzed by the chi-square and Fisher's exact tests and logistic regression. The Kaplan-Meier method including the log rank test was used to compare survival and recurrence.
RESULTS
Eight patients did not complete their treatment and were excluded from the study. We evaluated treatment responses and outcomes in 102 patients. Seventy-nine patients (77.5%) responded fully to chemotherapy while 23 patients (22.5%) required surgery. Among 23 patients who underwent surgery, 10 cases (43.5%) had bleeding, and 13 cases (56.5%) had drug resistance. Several factors were found to be significantly different between the groups who responded to chemotherapy and those who needed surgery, including age (p=0.001), antecedent non-molar pregnancy (0.028), tumor stage (p=0.009), and pre-treatment risk scores (p=0.008). But, the total courses of chemotherapy (p=0.521), need to salvage chemotherapy (p=0.074), survival rates (p=0.714), and disease free survival rates (p=0.206) were not significantly different.
CONCLUSION
The data suggest that age, antecedent non-molar pregnancy, tumor stage and the prognostic score are clinical predictors of need for surgery. But, it dose not seem that surgery have any effect on the total course of chemotherapy, need for salvage chemotherapy, and patient prognosis.
Keyword
MeSH Terms
Figure
-
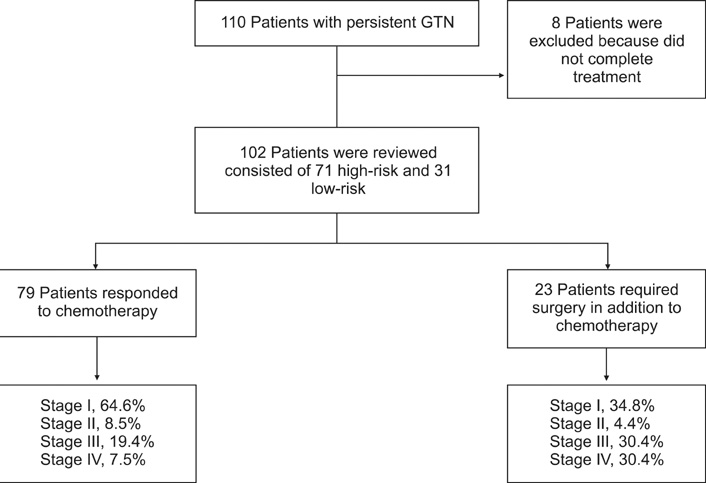
Fig. 1 Follow-up diagram of the study. GTN, gestational trophoblastic neoplasia.
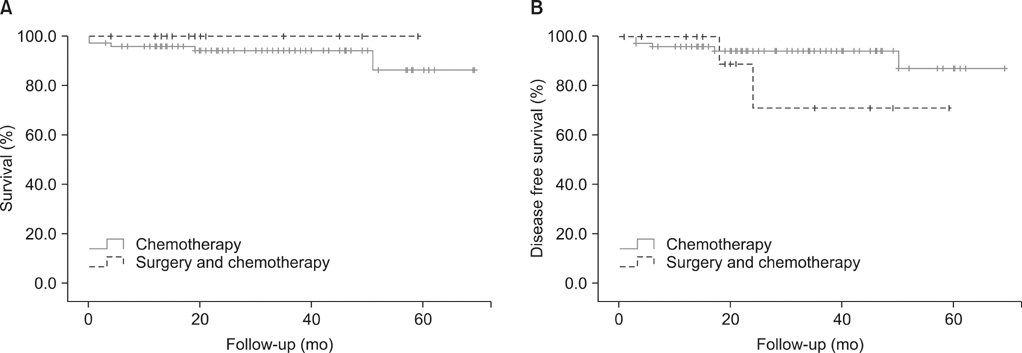
Fig. 2 (A) Kaplan-Meier curves of overall survival according to type of treatment. (B) Kaplan-Meier curves of disease-free survival according to type of treatment.
Reference
-
1. Altieri A, Franceschi S, Ferlay J, Smith J, La Vecchia C. Epidemiology and aetiology of gestational trophoblastic diseases. Lancet Oncol. 2003. 4:670–678.2. Ghaemmaghami F, Ashraf-Ganjooie T. Gestational trophoblastic neoplasia. Asia Pac J Clin Oncol. 2006. 2:9–21.3. Ngan HY. The practicability of FIGO 2000 staging for gestational trophoblastic neoplasia. Int J Gynecol Cancer. 2004. 14:202–205.4. Newlands ES. The management of recurrent and drug-resistant gestational trophoblastic neoplasia (GTN). Best Pract Res Clin Obstet Gynaecol. 2003. 17:905–923.5. Ghaemmaghami F, Behtash N, Soleimani K, Hanjani P. Management of patients with metastatic gestational trophoblastic tumor. Gynecol Oncol. 2004. 94:187–190.6. El-Lamie IK, Shehata NA, Abou-Loz SK, Ei-Lamie KI. Experience of the Gynecologic Oncology Unit at Ain Shams University in the treatment of gestational trophoblastic tumors. Int J Gynecol Cancer. 2000. 10:488–496.7. Soper J, Creasman WT. Disaia PJ, Creasman WT, editors. Gestational trophoblastic disease. Clinical gynecologic oncology. 2007. 7th ed. Philadelphia: Mosby Elsevier;201–230.8. Pisal N, North C, Tidy J, Hancock B. Role of hysterectomy in management of gestational trophoblastic disease. Gynecol Oncol. 2002. 87:190–192.9. Lurain JR, Singh DK, Schink JC. Role of surgery in the management of high-risk gestational trophoblastic neoplasia. J Reprod Med. 2006. 51:773–776.10. Tidy J. Hancock BW, Newlands ES, Berkowitz RS, Cole La, editors. The role of surgery in the management of gestational trophoblastic disease. Gestational trophoblastic diseases. 2009. 3rd ed. 430–446.11. Feltmate CM, Genest DR, Wise L, Bernstein MR, Goldstein DP, Berkowitz RS. Placental site trophoblastic tumor: a 17-year experience at the New England Trophoblastic Disease Center. Gynecol Oncol. 2001. 82:415–419.12. Gillespie AM, Liyim D, Goepel JR, Coleman RE, Hancock BW. Placental site trophoblastic tumour: a rare but potentially curable cancer. Br J Cancer. 2000. 82:1186–1190.13. Schmid P, Nagai Y, Agarwal R, Hancock B, Savage PM, Sebire NJ, et al. Prognostic markers and long-term outcome of placental-site trophoblastic tumours: a retrospective observational study. Lancet. 2009. 374:48–55.14. Balagopal P, Pandey M, Chandramohan K, Somanathan T, Kumar A. Unusual presentation of choriocarcinoma. World J Surg Oncol. 2003. 1:4.15. Berkowitz RS, Goldstein DP. Berek JS, Hacker NE, editors. Gestational trophoblastic neoplasia. Gynecologic oncology. 2010. 5th ed. Philadelphia: Williams & Wilkins;593–613.16. Newlands ES, Holden L, Seckl MJ, McNeish I, Strickland S, Rustin GJ. Management of brain metastases in patients with high-risk gestational trophoblastic tumors. J Reprod Med. 2002. 47:465–471.17. Feng F, Xiang Y, Li L, Wan X, Yang X. Clinical parameters predicting therapeutic response to surgical management in patients with chemotherapy-resistant gestational trophoblastic neoplasia. Gynecol Oncol. 2009. 113:312–315.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Epithelioid Trophoblastic Tumor in a Postmenopausal Woman: A Case Report
- Simplified Approach for Ovarian-Adnexal Reporting and Data System MRI Risk Stratification System
- Erratum to: Evaluation of sHLA-G levels in serum of patients with prostate cancer identify as a potential of tumor marker
- Treatment of Chemotherpay Resistant Lesion Localized on Lung in Gestational Trophoblastic Tumor.
- A Case of Persistent Gestational Trophoblastic Disease after Complete Hydatidiform Mole
