J Clin Neurol.
2009 Dec;5(4):167-172. 10.3988/jcn.2009.5.4.167.
Aggressive Glucose Control for Acute Ischemic Stroke Patients by Insulin Infusion
- Affiliations
-
- 1Department of Neurology, Eulji General Hospital, Eulji University College of Medicine, Seoul, Korea. nrkoomh@chol.com
- 2Department of Neurology, Dong-Eui Medical Center, Busan, Korea.
- 3Department of Biostatistics, Korea University College of Medicine, Seoul, Korea.
- KMID: 2287645
- DOI: http://doi.org/10.3988/jcn.2009.5.4.167
Abstract
- BACKGROUND AND PURPOSE
Hyperglycemia after acute ischemic stroke (AIS) is associated with poor outcomes. However, there is no consensus as to the optimal method for glycemic control. We designed an insulin infusion protocol for aggressive glucose control and investigated its efficacy and safety. METHODS: We applied our protocol to patients within 48 hours after AIS or transient ischemic attack (TIA) with an initial capillary glucose level of between 100 and 399 mg/dL (5.6-22.2 mmol/L). An insulin solution comprising 40 or 50 U of human regular insulin in 500 mL of 5% dextrose was administered for 24 hours. Capillary glucose was measured every 2 hours and the infusion rate was adjusted according to a nomogram with a target range of 80-129 mg/dL (4.4-7.2 mmol/L). Changes in glucose and overall glucose levels during insulin infusion were analyzed according to the presence of diabetes or admission hyperglycemia (admission glucose >139 mg/dL or 7.7 mmol/L) by the generalized estimating equation method. RESULTS: The study cohort comprised 115 consecutive patients. Glucose was significantly lowered from 160+/-57 mg/dL (8.9+/-3.2 mmol/L) at admission to 93+/-28 mg/dL (5.2+/-1.6 mmol/L) during insulin infusion (p<0.05). Laboratory hypoglycemia (capillary glucose <80 mg/dL or 4.4 mmol/L) occurred in 91 (71%) patients, 11 (10%) of whom had symptomatic hypoglycemia. Although glucose levels were significantly lowered and maintained within the target range in all patients, overall glucose levels were significantly higher in patients with diabetes or hyperglycemia (p<0.05). CONCLUSIONS: Our insulin-infusion protocol was effective in glycemic control for patients with AIS or TIA. Further modification is needed to improve the efficacy and safety of this procedure, and tailored intervention should be considered according to glycemic status.
Keyword
MeSH Terms
Figure
-
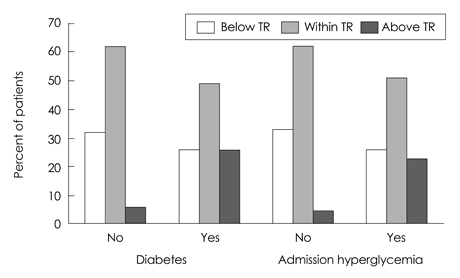
Fig. 1 The distribution of capillary glucose at 2 hours after insulin infusion with regard to target range (TR).
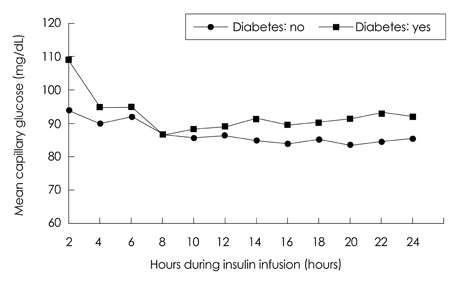
Fig. 2 Change of mean capillary glucose during insulin infusion according to the presence of diabetes.
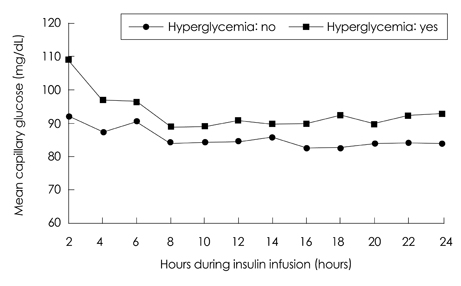
Fig. 3 Change of mean capillary glucose during insulin infusion according to the presence of admission hyperglycemia.
Reference
-
1. Capes SE, Hunt D, Malmberg K, Pathak P, Gerstein HC. Stress hyperglycemia and prognosis of stroke in nondiabetic and diabetic patients: a systematic overview. Stroke. 2001. 32:2426–2432.
Article2. Scott JF, Robinson GM, French JM, O'Connell JE, Alberti KG, Gray CS. Prevalence of admission hyperglycaemia across clinical subtypes of acute stroke. Lancet. 1999. 353:376–377.
Article3. Toni D, Sacchetti ML, Argentino C, Gentile M, Cavalletti C, Frontoni M, et al. Does hyperglycaemia play a role on the outcome of acute ischaemic stroke patients? J Neurol. 1992. 239:382–386.4. Quinn TJ, Lees KR. Hyperglycaemia in acute stroke--to treat or not to treat. Cerebrovasc Dis. 2009. 27:Suppl 1. 148–155.
Article5. Allport L, Baird T, Butcher K, Macgregor L, Prosser J, Colman P, et al. Frequency and temporal profile of poststroke hyperglycemia using continuous glucose monitoring. Diabetes Care. 2006. 29:1839–1844.
Article6. Baird TA, Parsons MW, Phanh T, Butcher KS, Desmond PM, Tress BM, et al. Persistent poststroke hyperglycemia is independently associated with infarct expansion and worse clinical outcome. Stroke. 2003. 34:2208–2214.
Article7. Kiers L, Davis SM, Larkins R, Hopper J, Tress B, Rossiter SC, et al. Stroke topography and outcome in relation to hyperglycaemia and diabetes. J Neurol Neurosurg Psychiatry. 1992. 55:263–270.
Article8. Weir CJ, Murray GD, Dyker AG, Lees KR. Is hyperglycaemia an independent predictor of poor outcome after acute stroke? Results of a long-term follow up study. BMJ. 1997. 314:1303–1306.
Article9. Williams LS, Rotich J, Qi R, Fineberg N, Espay A, Bruno A, et al. Effects of admission hyperglycemia on mortality and costs in acute ischemic stroke. Neurology. 2002. 59:67–71.
Article10. Gentile NT, Seftchick MW, Huynh T, Kruus LK, Gaughan J. Decreased mortality by normalizing blood glucose after acute ischemic stroke. Acad Emerg Med. 2006. 13:174–180.
Article11. Bhalla A, Wolfe CD, Rudd AG. Management of acute physiological parameters after stroke. QJM. 2001. 94:167–172.
Article12. Stead LG, Gilmore RM, Bellolio MF, Mishra S, Bhagra A, Vaidyanathan L, et al. Hyperglycemia as an independent predictor of worse outcome in non-diabetic patients presenting with acute ischemic stroke. Neurocrit Care. 2009. 10:181–186.
Article13. Farrokhnia N, Björk E, Lindbäck J, Terent A. Blood glucose in acute stroke, different therapeutic targets for diabetic and non-diabetic patients? Acta Neurol Scand. 2005. 112:81–87.
Article14. Clinical Research Center for Stroke. Available at: http://www.strokecrc.or.kr/.15. European Stroke Organisation (ESO) Executive Committee. ESO Writing Committee. Guidelines for management of ischaemic stroke and transient ischaemic attack 2008. Cerebrovasc Dis. 2008. 25:457–507.16. Adams HP Jr, del Zoppo G, Alberts MJ, Bhatt DL, Brass L, Furlan A, et al. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: the American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke. 2007. 38:1655–1711.
Article17. Bruno A, Kent TA, Coull BM, Shankar RR, Saha C, Becker KJ, et al. Treatment of hyperglycemia in ischemic stroke (THIS): a randomized pilot trial. Stroke. 2008. 39:384–389.18. Bruno A, Saha C, Williams LS, Shankar R. IV insulin during acute cerebral infarction in diabetic patients. Neurology. 2004. 62:1441–1442.
Article19. Gray CS, Hildreth AJ, Sandercock PA, O'Connell JE, Johnston DE, Cartlidge NE, et al. Glucose-potassium-insulin infusions in the management of post-stroke hyperglycaemia: the UK Glucose Insulin in Stroke Trial (GIST-UK). Lancet Neurol. 2007. 6:397–406.
Article20. Walters MR, Weir CJ, Lees KR. A randomised, controlled pilot study to investigate the potential benefit of intervention with insulin in hyperglycaemic acute ischaemic stroke patients. Cerebrovasc Dis. 2006. 22:116–122.
Article21. Zhu CZ, Auer RN. Optimal blood glucose levels while using insulin to minimize the size of infarction in focal cerebral ischemia. J Neurosurg. 2004. 101:664–668.
Article22. Fuentes B, Castillo J, San José B, Leira R, Serena J, Vivancos J, et al. The prognostic value of capillary glucose levels in acute stroke: the GLycemia in Acute Stroke (GLIAS) study. Stroke. 2009. 40:562–568.
Article23. Bruno A, Biller J, Adams HP Jr, Clarke WR, Woolson RF, Williams LS, et al. Acute blood glucose level and outcome from ischemic stroke. Trial of ORG 10172 in Acute Stroke Treatment (TOAST) Investigators. Neurology. 1999. 52:280–284.
Article24. Gray CS, Hildreth AJ, Alberti GK, O'Connell JE. GIST Collaboration. Poststroke hyperglycemia: natural history and immediate management. Stroke. 2004. 35:122–126.25. Alvarez-Sabin J, Molina CA, Montaner J, Arenillas JF, Huertas R, Ribo M, et al. Effects of admission hyperglycemia on stroke outcome in reperfused tissue plasminogen activator--treated patients. Stroke. 2003. 34:1235–1241.
Article26. Bruno A, Levine SR, Frankel MR, Brott TG, Lin Y, Tilley BC, et al. Admission glucose level and clinical outcomes in the NINDS rt-PA Stroke Trial. Neurology. 2002. 59:669–674.
Article27. Els T, Klisch J, Orszagh M, Hetzel A, Schulte-Mönting J, Schumacher M, et al. Hyperglycemia in patients with focal cerebral ischemia after intravenous thrombolysis: influence on clinical outcome and infarct size. Cerebrovasc Dis. 2002. 13:89–94.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Hemoperitoneum after Intraarterial Urokinase Infusion for Acute Ischemic Stroke
- Induced Hypertension Using Phenylephrine in Patients with Acute Ischemic Stroke: A Case Report
- Antiplatelet Therapy for Secondary Stroke Prevention in Patients with Ischemic Stroke or Transient Ischemic Attack
- Measurement of Insulin Sensitivity Index Estimated from LDIGIT ( Continuous Low Dose Insulin and Glucose Infusion Test
- Glycemic control in acute illness
