Hearing Performance Benefits of a Programmable Power Baha(R) Sound Processor with a Directional Microphone for Patients with a Mixed Hearing Loss
- Affiliations
-
- 1Department of Research and Applications, Cochlear Bone Anchored Solutions, Gothenburg, Sweden. mflynn@cochlear.com
Abstract
OBJECTIVES
New signal processing technologies have recently become available for Baha(R) sound processors. These technologies have led to an increase in power and to the implementation of directional microphones. For any new technology, it is important to evaluate the degree of benefit under different listening situations.
METHODS
Twenty wearers of the Baha osseointegrated hearing system participated in the investigation. The control sound processor was the Baha Intenso and the test sound processor was the Cochlear(TM) Baha(R) BP110power. Performance was evaluated in terms of free-field audibility with narrow band noise stimuli. Speech recognition of monosyllabic phonetically balanced (PB) words in quiet was performed at three intensity settings (50, 65, and 80 dB sound pressure level [SPL]) with materials presented at 0 degrees azimuth. Speech recognition of sentences in noise using the Hearing in Noise Test (HINT) in an adaptive framework was performed with speech from 0 degrees and noise held constant at 65 dB SPL from 180 degrees. Testing was performed in both the omni and directional microphone settings. Loudness growth was assessed in randomly presented 10 dB steps between 30 and 90 dB SPL to narrow band noise stimuli at 500 Hz and 3,000 Hz.
RESULTS
The test sound processor had significantly improved high frequency audibility (3,000-8,000 Hz). Speech recognition of PB words in quiet at three different intensity levels (50, 65, and 80 dB SPL) indicated a significant difference in terms of level (P<0.0001) but not for sound processor type (P>0.05). Speech recognition of sentences in noise demonstrated a 2.5 dB signal-to-noise ratio (SNR) improvement in performance for the test sound processor. The directional microphone provided an additional 2.3 dB SNR improvement in speech recognition (P<0.0001). Loudness growth functions demonstrated similar performance, indicating that both sound processors had sufficient headroom and amplification for the required hearing loss.
CONCLUSION
The test sound processor demonstrated significant improvements in the most challenging listening situation (speech recognition in noise). The implementation of a directional microphone demonstrated a further potential improvement in hearing performance. Both the control and test sound processors demonstrated good performance in terms of audibility, word recognition in quiet and loudness growth.
Keyword
MeSH Terms
Figure
-
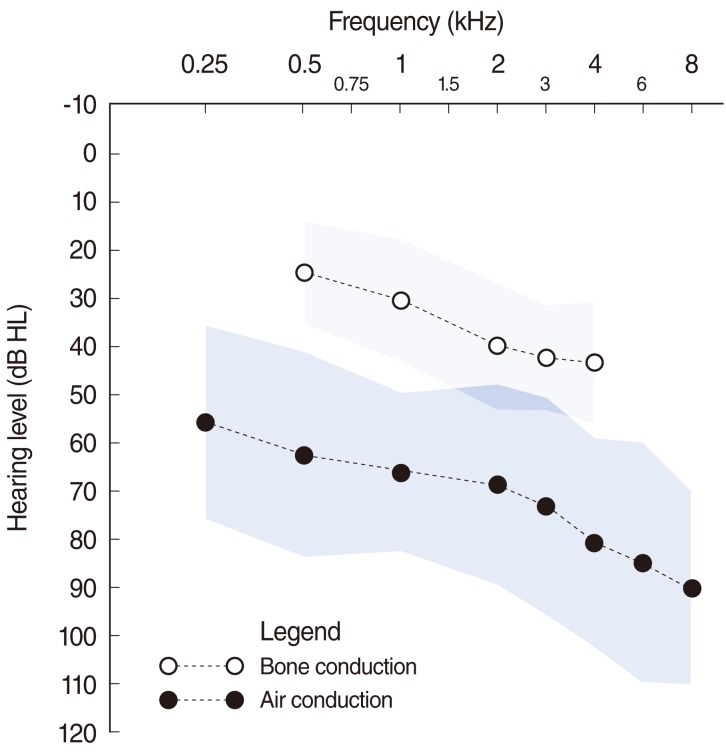
Fig. 1 Mean bone conduction and air conduction thresholds for the study participants demonstrating the mixed hearing loss. The shaded area highlights one standard deviation of the mean.
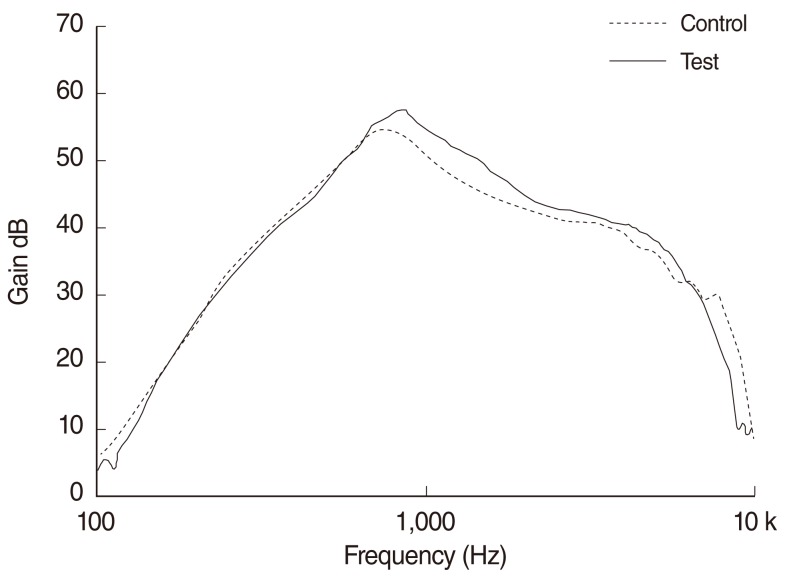
Fig. 2 Comparison of the maximum gain between the control and test sound processors. Due to improved design and feedback, the available gain in the test sound processor is higher across the mid frequencies by approximately 5 dB.
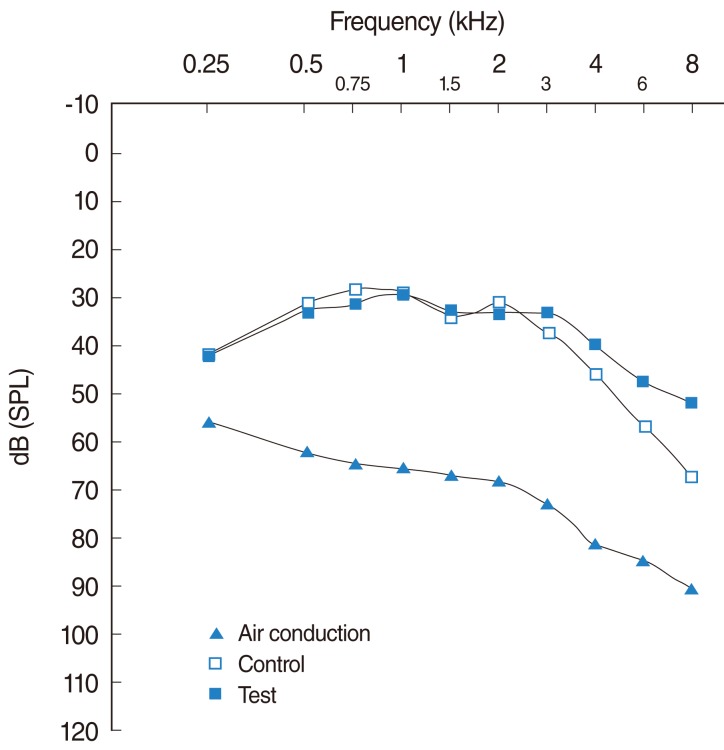
Fig. 3 Free-field aided thresholds (dB sound pressure level, SPL) as measured for the control and test sound processor. The differences from 3,000 to 8,000 were statistically significant (P<0.05). The air conduction values are also displayed to provide an indication of the overall degree of functional gain.
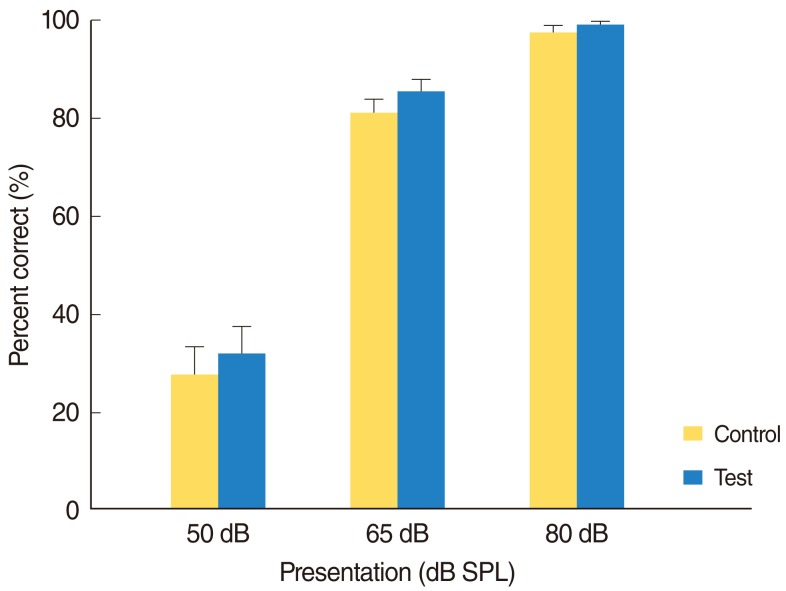
Fig. 4 Comparison of percentage correct for phonetically balanced words presented in quiet at three presentation levels for the control and test sound processors. Error bars equal one standard error of the mean. There was a significant difference (P<0.0001) in terms of level but not for sound processor type (P>0.05). SPL, sound pressure level.
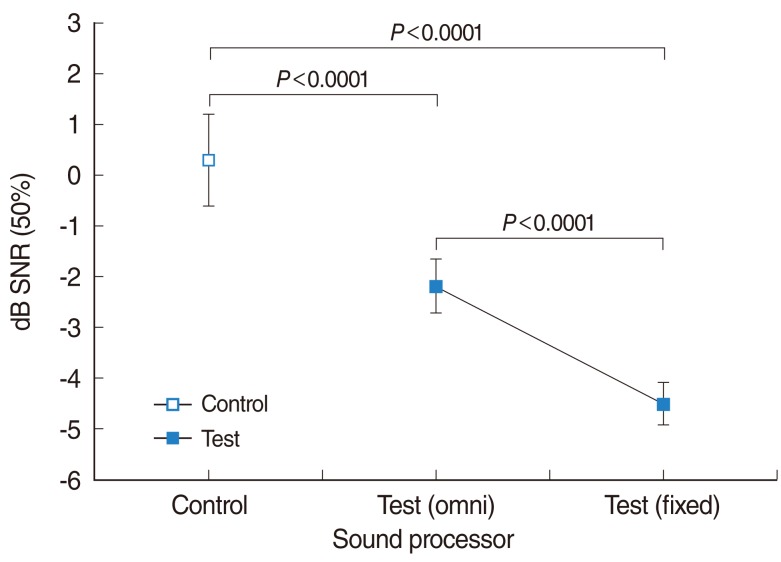
Fig. 5 Comparison of speech recognition in noise performance of the control and test sound processors demonstrating a 2.5 dB mean improvement in signal-to-noise ratio (SRN; P<0.0001). Comparison of the omni-directional and directional microphone in the test sound processor showed a further 2.3 dB advantage in speech recognition in noise (P<0.0001). Error bars indicate one standard error. Better performance is indicated by 50% performance in a poorer SNR.
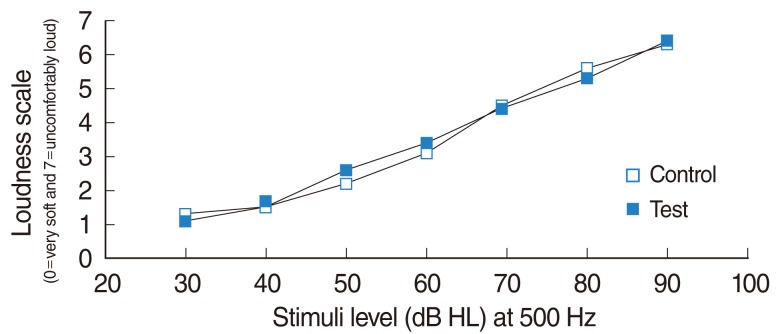
Fig. 6 Loudness growth measurements at 500 Hz for the control and test sound processors.
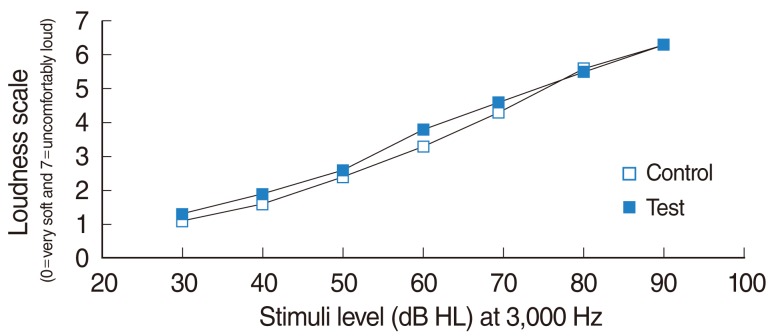
Fig. 7 Loudness growth measurements at 3,000 Hz for the control and test sound processors.
Reference
-
1. Bosman AJ, Snik FM, Mylanus EA, Cremers WR. Fitting range of the Baha Intenso. Int J Audiol. 2009; 48(6):346–352. PMID: 19925342.
Article2. Wazen JJ, Van Ess MJ, Alameda J, Ortega C, Modisett M, Pinsky K. The Baha system in patients with single-sided deafness and contralateral hearing loss. Otolaryngol Head Neck Surg. 2010; 4. 142(4):554–559. PMID: 20304277.
Article3. Flynn MC, Sadeghi A, Halvarsson G. Baha solutions for patients with severe mixed hearing loss. Cochlear Implants Int. 2009; 10(Suppl 1):43–47. PMID: 19195004.
Article4. De Wolf MJ, Hendrix S, Cremers CW, Snik AF. Better performance with bone-anchored hearing aid than acoustic devices in patients with severe air-bone gap. Laryngoscope. 2011; 3. 121(3):613–616. PMID: 21344443.
Article5. Davison T, Leese D, Marley S, Johnson IJ. Clinical impressions of a new Bone Anchored Hearing Aid processor. In : 2nd International Symposium on Bone Conduction Hearing - Craniofacial Osseointegration; 2009 Jun 11-13; Goteborg, Sweden.6. Flynn MC, Sadeghi A, Halvarsson G. Benefits of directional microphones and noise reduction circuits for improving Baha hearing performance. Cochlear Implants Int. 2011; 5. 12(Suppl 1):S139–S141. PMID: 21756499.7. Flynn MC. Challenges and recent developments in sound processing for Baha. Adv Otorhinolaryngol. 2011; 71:112–123. PMID: 21389711.8. Pfiffner F, Caversaccio MD, Kompis M. Comparisons of sound processors based on osseointegrated implants in patients with conductive or mixed hearing loss. Otol Neurotol. 2011; 7. 32(5):728–735. PMID: 21646934.
Article9. Snik AF, Mylanus EA, Proops DW, Wolfaardt JF, Hodgetts WE, Somers T, et al. Consensus statements on the Baha system: where do we stand at present? Ann Otol Rhinol Laryngol Suppl. 2005; 12. 195:2–12. PMID: 16619473.
Article10. Cochlear Bone Anchored Solutions. Verification protocol, G3 power (9228). 2011. Molnlycke, Sweden: Cochlear Bone Anchored Solutions.11. Cochlear Bone Anchored Solutions. G3 power verification record. 2011. Molnlycke, Sweden: Cochlear Bone Anchored Solutions.12. Cochlear Bone Anchored Solutions. G3 power PS4 verification test report. 2011. Molnlycke, Sweden: Cochlear Bone Anchored Solutions.13. Cochlear Bone Anchored Solutions. Baha fitting guide for professionals (E81231). 2008. Molnlykke, Sweden: Cochlear Bone Anchored Solutions.14. Flynn MC, Sammeth CA, Sadeghi A, Cire G, Halvarsson G. Baha for single-sided sensorineural deafness: review and recent technological innovations. Semin Hear. 2010; 11. 31(4):326–349.
Article15. Andrew R, Green KM. Unilateral conductive and sensorineural hearing loss with BC direct. Audiol Neurootol. 2011; 16(Suppl 1):23–25. PMID: 20516679.16. Liden G. Speech audiometry; an experimental and clinical study with Swedish language material. Acta Otolaryngol Suppl. 1954; 114:1–145. PMID: 13147805.17. Liden G, Fant G. Swedish word material for speech audiometry and articulation tests. Acta Otolaryngol Suppl. 1954; 116:189–204. PMID: 13188683.18. Arlinger S. Nu finns testlistor pa CD. AudioNytt. 1988; 15(3):4–5.19. Hallgren M, Larsby B, Arlinger S. A Swedish version of the Hearing In Noise Test (HINT) for measurement of speech recognition. Int J Audiol. 2006; 4. 45(4):227–237. PMID: 16684704.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Acceptable Noise Level Benefit From Directionality for Listeners With Severe Hearing Loss
- Middle Ear Implant
- Experience of BAHA(Bone Anchored Hearing Aid) Surgery
- Improving the Accuracy of Baha(R) Fittings through Measures of Direct Bone Conduction
- Advantages of Binaural Amplification to Acceptable Noise Level of Directional Hearing Aid Users
