The Usefulness of Reconstructed 3D Images in Surgical Planning for Cochlear Implantation in a Malformed Ear with an Abnormal Course of the Facial Nerve
- Affiliations
-
- 1Department of Otorhinolaryngology Head and Neck Surgery, Nagasaki University Hospital, Nagasaki, Japan. harami@nagasaki-u.ac.jp
- 2Kanda ENT Clinic, Nagasaki Bell Hearing Center, Nagasaki, Japan.
Abstract
OBJECTIVES
It is not unusual for a cochlear implantation (CI) candidate to have some type of ear malformation, in particular an abnormal course of the facial nerve (FN). In this study, we attempted to reconstruct a three-dimensional (3D) image of temporal bone structures with malformation using computed tomography (CT) imaging and examined its usefulness in the surgical planning of CI in a malformed ear.
METHODS
We prepared 3D images for 6 separate CI cases before surgery. First, we manually colored preoperative CT images using Photoshop CS Extended. We then converted the colored CT images to 3D images using Delta Viewer, free-ware for Macintosh. Before surgery, we discussed any problems anticipated based on the 3D images and plans for surgery with those who would be performing the CI.
RESULTS
Case 1: The subject was a 3-year-old boy with malformed ossicles, semicircular canal (SC) hypoplasia, internal auditory canal stenosis, and an abnormal course of the FN. 3D image indicated that the stapes were absent, and the FN was more anteriorly displaced, so that it was difficult to perform cochleostomy. The surgical findings were similar to those depicted on the 3D image, so we could insert an electrode based on the preoperative image simulation without complications. Case 2: The subject was a 7-year-old boy with malformed stapes, atresia of the round window, cochlear and SC aplasia, and an abnormal course of the FN with bifurcation. CI was performed with no problems, in the same manner as in Case 1.
CONCLUSION
We were able to successfully depict the structures of the inner ear, ossicles, and FN as 3D images, which are very easy to understand visually and intuitively. These 3D images of the malformed ear are useful in preoperative image simulation and in surgical planning for those performing a CI procedure.
MeSH Terms
Figure
-

Fig. 1 Example of Delta Viewer 3 dimensional image of normal temporal bone structures of left ear based on computed tomography image. Image (A) is antero-lateral inferior view, and image (B) is superior view. The bony labyrinth was shaded in blue and includes the cochlea (Co), vestibule (V), anterior semicircular canal (ASC), lateral semicircular canal (LSC), posterior semicircular canal (PSC), and round window (RW). The internal auditory canal (IAC) and facial nerve (FN) are shaded in yellow. The ossicles are shaded in red and include the malleus (M), incus (I), and stapes (S). The annulus tympanicus (AT) and vestibular aqueduct (VA) are shaded in green and purple, respectively.
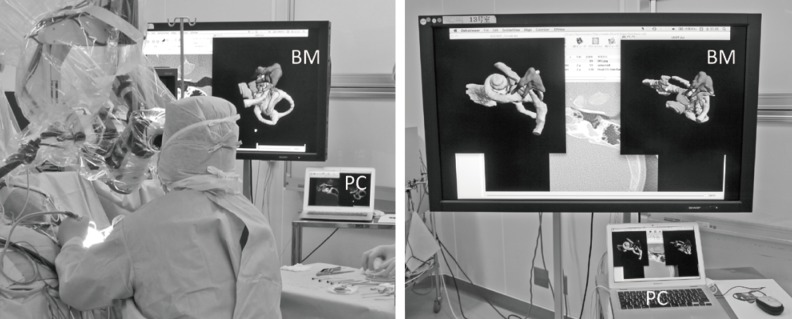
Fig. 2 The pictures of an operation room during a cochlear implantation surgery. The surgeon sees Delta Viewer 3 dimensional images displayed on the bedside monitor (BM), which is controlled by the notebook PC (Macintosh), and compares the images with surgical findings.

Fig. 3 (A) Lateral view of the temporal bone structures of case 1. The lateral semicircular canal (LSC) is hypoplastic, and the crus of the incus (I) and stapes (S) are absent. The labyrinthine segment of the facial nerve (FN) and the geniculate ganglion are posteriorly displaced, and the tympanic and mastoid segments of the FN are antero-inferiorly displaced, running more vertically than normal control. The cochlea (Co), malleus (M), anterior semicircular canal (ASC), and posterior semicircular canal (PSC) are intact. (B) Lateral view of normal control. The green arrowhead shows the course of the FNs.

Fig. 4 (A) The Delta Viewer 3 dimensional (DV-3D) image of case 1 in the same position during cochlear implantation surgery. (B) The DV-3D image of normal control in the same position as (A). Rectangle of dashed line shows the area of Fig. 5. Co, cochlea; ASC, anterior semicircular canal; PSC, posterior semicircular canal; LSC, lateral semicircular canal; FN, facial nerve; M, malleus; I,incus; S, stapes.
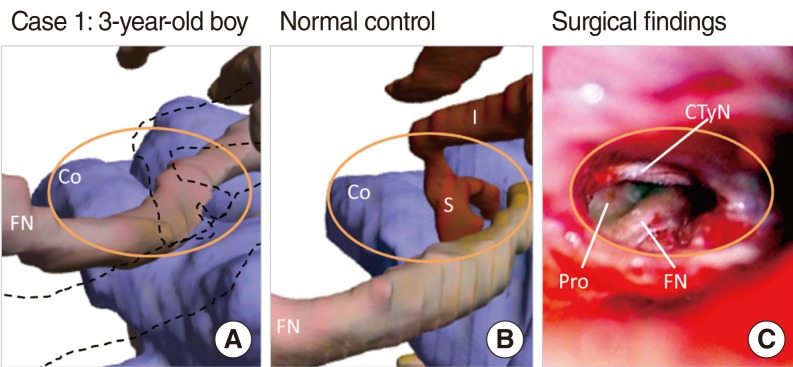
Fig. 5 The images of the surgical field of posterior tympanotomy as shown by the orange oval. (A) Case 1: close-up image of the rectangle of Fig. 4A. The stapes (S) and crus of the incus (I) are absent, and the facial nerve (FN) is antero-inferiorly displaced. Dashed line shows the position of the ossicles and facial nerve (FN) of normal control. The visible area of the basal turn of cochlea (Co) is smaller than normal. (B) Normal control: close-up image of the rectangle of Fig.4B. (C) The picture of the surgical findings of case 1. The visible area of the promontory (Pro) for cochleostomy is narrow and surrounded by the chorda tympani nerve (CTyN) and facial nerve (FN) displaced anteriorly.

Fig. 6 The X-ray of inserted electrode of case 1.
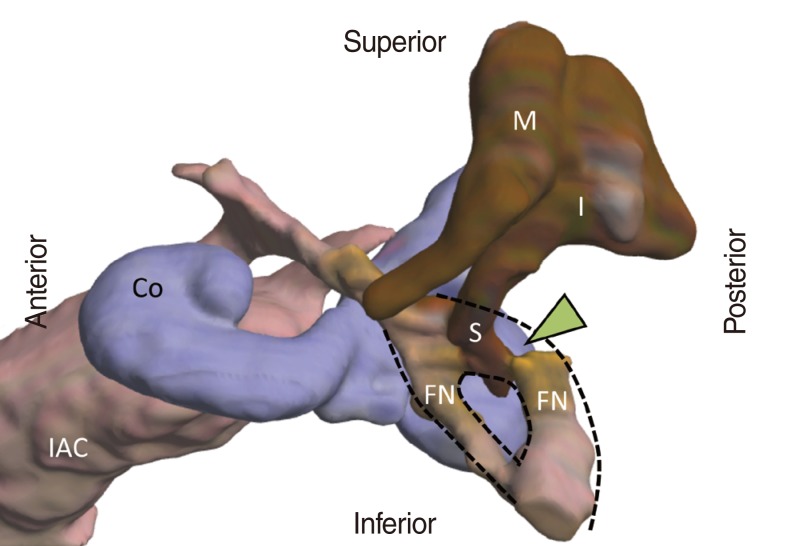
Fig. 7 Antero-lateral view of the temporal bone structures of case 2. The shape of the cochlea (Co) and semicircular canals are hypoplastic. The labyrinthine segment of the facial nerve (FN) and geniculate ganglion are posteriorly displaced, the tympanic and mastoid segments of the FN are antero-inferiorly displaced with bifurcation, and the stapes is fused to the facial nerve (arrow head). IAC, internal auditory canal; M,malleus; I, incus; S, stapes.
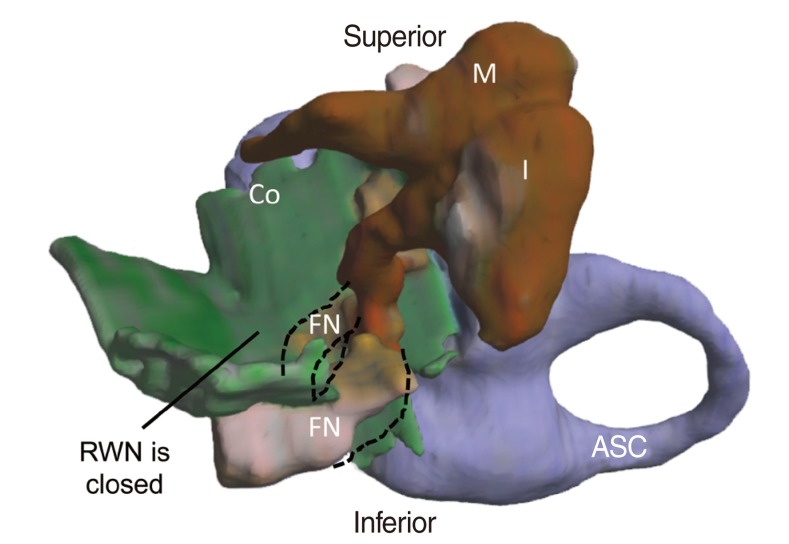
Fig. 8 The Delta Viewer 3 dimensional image of case 2 in the same position during cochlear implantation surgery. The surface of the tympanic cavity is displayed in green. The round window niche (RWN) is closed, so there was no landmark for cochlear fenestration. Co, cochlea; FN, facial nerve; ASC, anterior semicircular canal; M, malleus; I, incus.

Fig. 9 The X-ray of inserted electrode of case 2.
Reference
-
1. Fujii N, Inui Y, Katada K. Temporal bone anatomy: correlation of multiplanar reconstruction sections and three-dimensional computed tomography images. Jpn J Radiol. 2010; 11. 28(9):637–648. PMID: 21113747.
Article2. Sorensen MS, Dobrzeniecki AB, Larsen P, Frisch T, Sporring J, Darvann TA. The visible ear: a digital image library of the temporal bone. ORL J Otorhinolaryngol Relat Spec. 2002; Nov-Dec. 64(6):378–381. PMID: 12499759.3. Wang H, Merchant SN, Sorensen MS. A downloadable three-dimensional virtual model of the visible ear. ORL J Otorhinolaryngol Relat Spec. 2007; 69(2):63–67. PMID: 17124433.
Article4. Sorensen MS, Mosegaard J, Trier P. The visible ear simulator: a public PC application for GPU-accelerated haptic 3D simulation of ear surgery based on the visible ear data. Otol Neurotol. 2009; 6. 30(4):484–487. PMID: 19546800.5. Venail F, Deveze A, Lallemant B, Guevara N, Mondain M. Enhancement of temporal bone anatomy learning with computer 3D rendered imaging software. Med Teach. 2010; 32(7):e282–e288. PMID: 20653370.6. Mukherjee P, Uzun-Coruhlu H, Curthoys IS, Jones AS, Bradshaw AP, Pohl DV. Three-dimensional analysis of the vestibular end organs in relation to the stapes footplate and piston placement. Otol Neurotol. 2011; 4. 32(3):367–372. PMID: 21283036.
Article7. Noble JH, Dawant BM, Warren FM, Labadie RF. Automatic identification and 3D rendering of temporal bone anatomy. Otol Neurotol. 2009; 6. 30(4):436–442. PMID: 19339909.
Article8. McClerkin WW, Schuknecht HF. Facial nerve and stapes anomaly: a case report. Laryngoscope. 1974; 7. 84(7):1202–1209. PMID: 4841642.
Article9. Takahashi H, Kawanishi M, Maetani T. Abnormal branching of facial nerve with ossicular anomalies: report of two cases. Am J Otol. 1998; 11. 19(6):850–853. PMID: 9831167.10. Romo LV, Curtin HD. Anomalous facial nerve canal with cochlear malformations. AJNR Am J Neuroradiol. 2001; 5. 22(5):838–844. PMID: 11337325.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recurrent Meningitis in a Patient with Inner Ear Anomaly after Cochlear Implantation
- A Case of Cochlear Implantation in a Child with Congenital Aural Atresia and Cochlear and Cochlear Nerve Malformation
- Combined Endoscopic/Microscopic Cochlear Implantation Through the Oval Window
- Cochlear Implantation Using the Endomeatal Approach in a Child with a Extremely Hypoplastic Mastoid
- Cochlear Implantation Using a Suprameatal Approach in a Case of Severely Contracted Mastoid Cavity
