Syndromic Hearing Loss in Association with PTPN11-Related Disorder: The Experience of Cochlear Implantation in a Child with LEOPARD Syndrome
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. hongsh@skku.edu
- 2Department of Laboratory Medicine & Genetics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. heejinkim@skku.edu
Abstract
- Hearing loss (HL) is one of the most frequent clinical manifestations of patients who suffer with multi-systemic genetic disorders. HL in association with other physical stigmata is referred to as a syndromic form of HL. LEOPARD syndrome (LS) is one of the disorders with syndromic HL and it is caused by a mutation in the PTPN11 or RAF1 gene. In general, 5 year old children who undergo cochlear implantation usually show a marked change in behavior regarding sound detection within the first 6 months of implant use, but word identification may not be exhibited for at least another 6-12 months of implant use. We herein report on a 5-year-old girl with LS. Her clinical manifestations including bilateral sensorineural HL, which indicated the diagnosis of LS. We confirmed the diagnosis by identifying a disease-causing mutation in the PTPN11 gene, which was a heterozygous missense mutation Ala461Thr (c.1381G>A). She underwent cochlear implantation (CI) without complications and she is currently on regular follow-up at postoperative 1 year. This is the first reported case of CI in a patient with LS in the medical literature.
Keyword
MeSH Terms
Figure
-
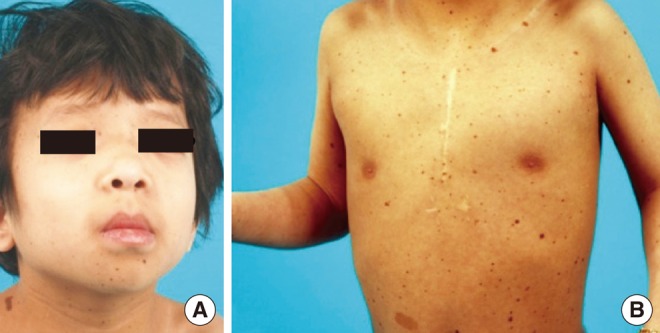
Fig. 1 The patient had hypertelorism, ptosis and low-set ears (A), and diffuse lentiginosis on the anterior trunk (B).
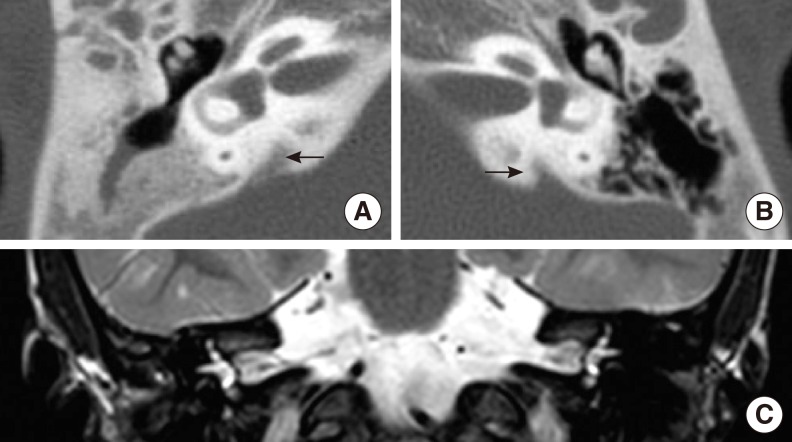
Fig. 2 Computed tomography (CT) of the temporal bone (A, B) and magnetic resonance imaging (MRI) of the internal auditory canal were performed (C). Bilateral enlarged vestibular aqueducts (arrow) were identified, but both of the internal auditory canals were observed to be of normal size. The cochlea and the semicircular canals were also of normal shape and filled with fluid on both sides. (A) temporal bone CT of the right side, (B) temporal bone CT of the left side, (C) T2 weighted MR coronal view image.
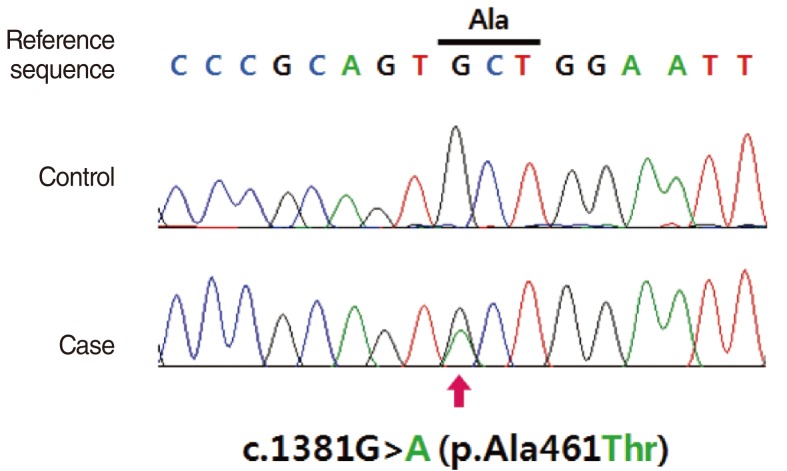
Fig. 3 The patient had a missense mutation in the PTPN11 gene (c.1381G>A, p.Ala461Thr) that was detected on direct sequencing analysis.
Reference
-
1. Gorlin RJ, Anderson RC, Blaw M. Multiple lentigenes syndrome. Am J Dis Child. 1969; 6. 117(6):652–662. PMID: 5771505.
Article2. Seuanez H, Mane-Garzon F, Kolski R. Cardio-cutaneous syndrome (the "LEOPARD" syndrome): review of the literature and a new family. Clin Genet. 1976; 3. 9(3):266–276. PMID: 1261064.
Article3. Digilio MC, Conti E, Sarkozy A, Mingarelli R, Dottorini T, Marino B, et al. Grouping of multiple-lentigines/LEOPARD and Noonan syndromes on the PTPN11 gene. Am J Hum Genet. 2002; 8. 71(2):389–394. PMID: 12058348.
Article4. Legius E, Schrander-Stumpel C, Schollen E, Pulles-Heintzberger C, Gewillig M, Fryns JP. PTPN11 mutations in LEOPARD syndrome. J Med Genet. 2002; 8. 39(8):571–574. PMID: 12161596.
Article5. Pandit B, Sarkozy A, Pennacchio LA, Carta C, Oishi K, Martinelli S, et al. Gain-of-function RAF1 mutations cause Noonan and LEOPARD syndromes with hypertrophic cardiomyopathy. Nat Genet. 2007; 8. 39(8):1007–1012. PMID: 17603483.
Article6. Voron DA, Hatfield HH, Kalkhoff RK. Multiple lentigines syndrome: case report and review of the literature. Am J Med. 1976; 3. 60(3):447–456. PMID: 1258892.7. Allanson JE, Hall JG, Van Allen MI. Noonan phenotype associated with neurofibromatosis. Am J Med Genet. 1985; 7. 21(3):457–462. PMID: 2411134.
Article8. Ahlbom BE, Dahl N, Zetterqvist P, Anneren G. Noonan syndrome with cafe-au-lait spots and multiple lentigines syndrome are not linked to the neurofibromatosis type 1 locus. Clin Genet. 1995; 8. 48(2):85–89. PMID: 7586657.9. Colley A, Donnai D, Evans DG. Neurofibromatosis/Noonan phenotype: a variable feature of type 1 neurofibromatosis. Clin Genet. 1996; 2. 49(2):59–64. PMID: 8740913.
Article10. Coppin BD, Temple IK. Multiple lentigines syndrome (LEOPARD syndrome or progressive cardiomyopathic lentiginosis). J Med Genet. 1997; 7. 34(7):582–586. PMID: 9222968.
Article11. Limongelli G, Pacileo G, Marino B, Digilio MC, Sarkozy A, Elliott P, et al. Prevalence and clinical significance of cardiovascular abnormalities in patients with the LEOPARD syndrome. Am J Cardiol. 2007; 8. 100(4):736–741. PMID: 17697839.
Article12. Limongelli G, Sarkozy A, Pacileo G, Calabro P, Digilio MC, Maddaloni V, et al. Genotype-phenotype analysis and natural history of left ventricular hypertrophy in LEOPARD syndrome. Am J Med Genet A. 2008; 3. 146A(5):620–628. PMID: 18241070.
Article13. Sarkozy A, Conti E, Digilio MC, Marino B, Morini E, Pacileo G, et al. Clinical and molecular analysis of 30 patients with multiple lentigines LEOPARD syndrome. J Med Genet. 2004; 5. 41(5):e68. PMID: 15121796.
Article14. Sarkozy A, Obregon MG, Conti E, Esposito G, Mingarelli R, Pizzuti A, et al. A novel PTPN11 gene mutation bridges Noonan syndrome, multiple lentigines/LEOPARD syndrome and Noonan-like/multiple giant cell lesion syndrome. Eur J Hum Genet. 2004; 12. 12(12):1069–1072. PMID: 15470362.15. Staller SJ, Beiter AL, Brimacombe JA. Use of the Nucleus 22 channel cochlear implant system with children. Volta Rev. 1994; 96:15–40.
