Non-cardiac Findings on 64-Slice Cardiac Multi-detector CT
- Affiliations
-
- 1Division of Cardiology, Seoul National University Bundang Hospital, Seongnam, Korea. hjchang@snu.ac.kr
- 2Division of Radiology, Seoul National University Bundang Hospital, Seongnam, Korea.
- KMID: 2225790
- DOI: http://doi.org/10.4070/kcj.2008.38.5.276
Abstract
-
BACKGROUND AND OBJECTIVES: Multi-detector CT (MDCT) is becoming more commonly used as a diagnostic tool for various cardiac diseases, and this modality can also incidentally detect a significant number of non-cardiac findings during cardiac work-ups. The objectives of this study were to evaluate the incidence of non-cardiac findings during cardiac MDCT and to compare them with chest CT.
SUBJECTS AND METHODS
We enrolled 1,007 consecutive subjects (mean age: 49+/-10 years, males: 63%) who underwent both cardiac and chest CT (64-slice MDCT) as a part of a routine health check-up. The subjects were evaluated for the incidence of non-cardiac findings and the therapeutic consequences according to the CT protocols during the mid-term follow-up (average length of mid-term follow-up: 533+/-39 days).
RESULTS
Eight hundred sixty incidental non-cardiac findings were identified in 627 patients (62%) with cardiac CT. Forty-three subjects (4%) had clinically significant lesions that required additional diagnostic work-up or radiological follow-up, and these lesions were 23 cases of non-calcified nodule, 2 cases of ground glass opacity, 6 cases of pneumonia, 1 case of active tuberculosis, 2 cases of focal bronchiolitis, 3 cases of arterial lesion, 1 case of liver cirrhosis and 5 cases of extra-pulmonary masses. Five subjects (0.5%), including 2 cases (0.2%) of malignancy, had therapeutic consequences during their follow-up. Compared with chest CT, 68% (40/59) of the significant intrathoracic lesions and 67% (4/6) of the intrathoracic lesions with therapeutic consequences were documented by cardiac CT.
CONCLUSION
In the present study, 4% of the asymptomatic patients who underwent cardiac MDCT were found to have significant non-cardiac findings that required further work-up. To avoid missing a number of clinically important findings, physicians who analyze cardiac MDCT scans should carefully evaluate not only the heart, but all the other organs that are within the scan range.
Keyword
MeSH Terms
Figure
-

Fig. 1 Field of views (FOV) for the cardiac and chest CT. A: the view in box A is the limited field of view that is conventionally used for the reconstruction of cardiac MDCT. B: the view in box B is the entire scan range for cardiac MDCT, that is, the maximal field of view for cardiac MDCT. C: the view in box C is the scan range for chest CT. MDCT: multi-detector CT.
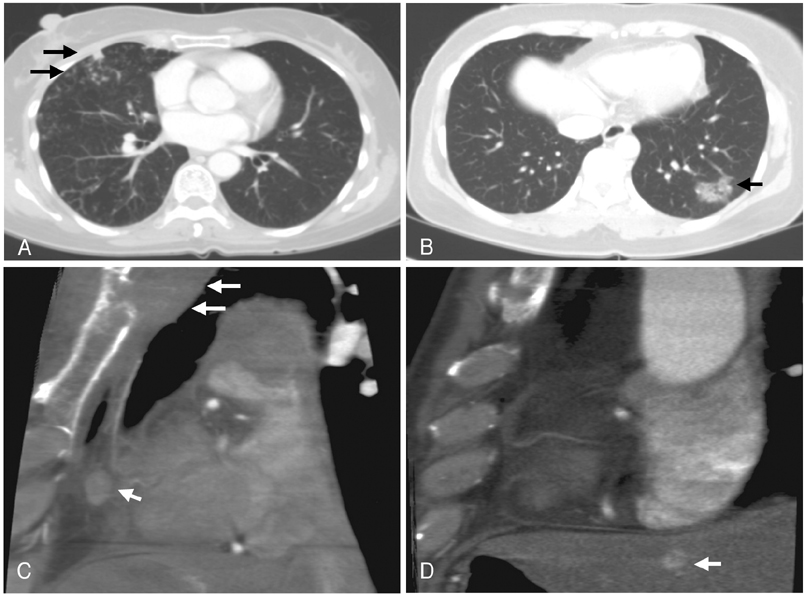
Fig. 2 Cases of significant non-cardiac findings on the maximal FOV of cardiac MDCT. A: a 53-year-old woman with mycobacteria other than tuberculosis (arrows). B: a 39-year-old woman with bronchiolitis obliterans organizing pneumonia (arrow). C: a 53-year-old man with thymic carcinoma that showed bone invasion (arrows) and metastatic spread to a lymph node (arrowhead). D: a 61-year-old man with hepatocellular carcinoma (arrow).
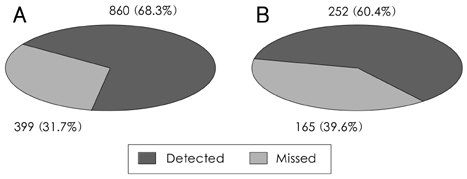
Fig. 3 Cardiac MDCT detection of non-cardiac findings on Chest CT (n=1007, per patient analysis). The graphic shows the proportion of non-cardiac findings detected on cardiac CT as compared with chest CT. A: overall lesions (n=1259). B: intrathoracic lesions (n=417).
Reference
-
1. Klingenbeck-Regn K, Schaller S, Flohr T, Ohnesorge B, Kopp AF, Baum U. Subsecond multi-slice computed tomography: basics and applications. Eur J Radiol. 1999. 31:110–124.2. Ohnesorge B, Flohr T, Becker C, et al. Cardiac imaging by means of electrocardiographically gated multisection spiral CT: initial experience. Radiology. 2000. 217:564–571.3. Mönninghoff W, Gradaus D, Bender F. The significance of coronary artery calcification seen by roentgenoscopy (author's transl). Z Kardiol. 1977. 66:10–14.4. Choe Y. Noninvasive imaging of atherosclerotic plaques using MRI and CT. Korean Circ J. 2005. 35:1–14.5. Becker CR, Ohnesorge BM, Schoepf UJ, Reiser MF. Current development of cardiac imaging with multidetector-row CT. Eur J Radiol. 2000. 36:97–103.6. Nieman K, Oudkerk M, Rensing BJ, et al. Coronary angiography with multi-slice computed tomography. Lancet. 2001. 357:599–603.7. Ropers D, Baum U, Pohle K, et al. Detection of coronary artery stenoses with thin-slice multi-detector row spiral computed tomography and multiplanar reconstruction. Circulation. 2003. 107:664–666.8. Oh HJ, Kwon K, Park SH, et al. CT coronary angiography using multidetector computed tomography in coronary artery disease: a comparative study to quantitive coronary angiography. Korean Circ J. 2004. 34:1167–1173.9. Kiyohara C, Yoshimasu K, Shirakawa T, Hopkin JM. Genetic polymorphisms and environmental risk of lung cancer: a review. Rev Environ Health. 2004. 19:15–38.10. Onuma Y, Tanabe K, Nakazawa G, et al. Noncardiac findings in cardiac imaging with multidetector computed tomography. J Am Coll Cardiol. 2006. 48:402–406.11. Haller S, Kaiser C, Buser P, Bongartz G, Bremerich J. Coronary artery imaging with contrast-enhanced MDCT: extracardiac findings. AJR Am J Roentgenol. 2006. 187:105–110.12. Gil BN, Ran K, Tamar G, Shmuell F, Eli A. Prevalence of significant noncardiac findings on coronary multidetector computed tomography angiography in asymptomatic patients. J Comput Assist Tomogr. 2007. 31:1–4.13. Budoff MJ, Achenbach S, Fayad Z, et al. Task Force 12: training in advanced cardiovascular imaging (computed tomography): endorsed by the American Society of Nuclear Cardiology, Society for Cardiovascular Angiography and Interventions, Society of Atherosclerosis Imaging and Prevention, and Society of Cardiovascular Computed Tomography. J Am Coll Cardiol. 2006. 47:915–920.14. Budoff MJ, Fischer H, Gopal A. Incidental findings with cardiac CT evaluation: should we read beyond the heart? Catheter Cardiovasc Interv. 2006. 68:965–973.15. Rumberger JA. Noncardiac abnormalities in diagnostic cardiac computed tomography: within normal limits or we never looked! J Am Coll Cardiol. 2006. 48:407–408.16. Hendel RC, Patel MR, Kramer CM, et al. ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 appropriateness criteria for cardiac computed tomography and cardiac magnetic resonance imaging: a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, American College of Radiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American Society of Nuclear Cardiology, North American Society for Cardiac Imaging, Society for Cardiovascular Angiography and Interventions, and Society of Interventional Radiology. J Am Coll Cardiol. 2006. 48:1475–1497.17. Wilck EJ. Computed tomography screening for lung cancer. Ann Thorac Surg. 2008. 85:S699–S700.18. Semelka RC, Armao DM, Elias J Jr, Huda W. Imaging strategies to reduce the risk of radiation in CT studies, including selective substitution with MRI. J Magn Reson Imaging. 2007. 25:900–909.19. Einstein AJ, Henzlova MJ, Rajagopalan S. Estimating risk of cancer associated with radiation exposure from 64-slice computed tomography coronary angiography. JAMA. 2007. 298:317–323.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Diagnostic accuracy of 64-slice multi-detector CT coronary angiography in the evaluation of coronary artery disease
- Incidental Non-Cardiac Findings of a Coronary Angiography with a 128-Slice Multi-Detector CT Scanner: Should We Only Concentrate on the Heart?
- 16-Slice Multi-Detector Row CT Coronary Angiography: Image Quality and Optimization of the Image Reconstruction Window
- Multi-Slice Spiral CT of Living-Related Liver Transplantation in Children: Pictorial Essay
- The Diagnostic Accuracy of the 64-slice Multi-detector CT Coronary Angiography for the Assessment of Coronary Artery Stenosis in Symptomatic Patients
