Korean Circ J.
2011 Feb;41(2):61-67. 10.4070/kcj.2011.41.2.61.
Effect of Valsartan on N-Terminal Pro-Brain Natriuretic Peptide in Patient With Stable Chronic Heart Failure: Comparison With Enalapril
- Lee YS
- Kim KS
- Lee JB
- Ryu JK
- Choi JY
- Kim BK
- Chang SG
- Hur SH

- Lee BR
- Jung BC
- Hong GR
- Kim BS
- Park TH
- Kim YD
- Kim TI
- Kim DS
- Affiliations
-
- 1Department of Cardiology, Catholic University of Daegu, Daegu, Korea. kks7379@cu.ac.kr
- 2Institute for Atherosclerosis and CVD, Catholic University of Daegu, Daegu, Korea.
- 3Department of Cardiology, Keimyung University College of Medicine, Daegu, Korea.
- 4Department of Cardiology, Fatima General Hospital, Daegu, Korea.
- 5Department of Cardiology, Yeungnam University College of Medicine, Daegu, Korea.
- 6Department of Cardiology, DaeDong Hospital, Busan, Korea.
- 7Department of Cardiology, Dong-A University College of Medicine, Busan, Korea.
- 8Department of Cardiology, Maryknoll Medical Center, Busan, Korea.
- 9Department of Cardiology, Busan Paik Hospital, Busan, Korea.
- KMID: 2225137
- DOI: http://doi.org/10.4070/kcj.2011.41.2.61
Abstract
- BACKGROUND AND OBJECTIVES
The plasma concentration of N-terminal pro-brain natriuretic peptide (NT-pro-BNP) is a st-rong prognostic indicator for patients with heart failure (HF) across all stages of the condition. Several clinical trials have de-monstrated convincingly that neurohormonal modulation on the renin angiotensin system (RAS) decreases plasma NT-pro-BNP level and results in favorable outcomes. But there are still limited comparative data on the neuro-hormonal modulatory effects of two RAS inhibitors: angiotensin converting enzyme inhibitor and angiotensin receptor blocker.
SUBJECTS AND METHODS
This study was a prospective, multi-center, randomized, open-label, controlled, and non-inferiority study involving 445 patients with left ventricular ejection fraction (LVEF) less than 45%. Patients were assigned to receive either valsartan (target dose of 160 mg bid) or enalapril (target dose of 10 mg bid) for 12 months. We compared plasma NT-pro-BNP, high sensitive C-reactive protein (hs-CRP) level and echocardiographic parameters before and after treatment with valsartan or enalapril.
RESULTS
The NT-pro-BNP and hs-CRP levels were significantly decreased after 12 months of treatment with valsartan and enalapril. The percentage change was similar between both groups. LVEF improved and left ventricular internal dimensions were decreased in both groups, and there were no significant differences between two groups.
CONCLUSION
Valsartan is as effective on improving plasma NT-pro-BNP level as enalapril in patients with stable chronic HF.
Keyword
MeSH Terms
-
Angiotensin-Converting Enzyme Inhibitors
Angiotensins
C-Reactive Protein
Enalapril
Heart
Heart Failure
Humans
Natriuretic Peptide, Brain
Peptidyl-Dipeptidase A
Plasma
Prospective Studies
Renin-Angiotensin System
Stroke Volume
Tetrazoles
Valine
Valsartan
Angiotensin-Converting Enzyme Inhibitors
Angiotensins
C-Reactive Protein
Enalapril
Natriuretic Peptide, Brain
Peptidyl-Dipeptidase A
Tetrazoles
Valine
Figure
-

Fig. 1 Study design. TTE: transthoracic echocardiography, NT-pro-BNP: N-terminal pro-brain natriuretic peptide, hs-CRP: high sensitive C-reactive protein.
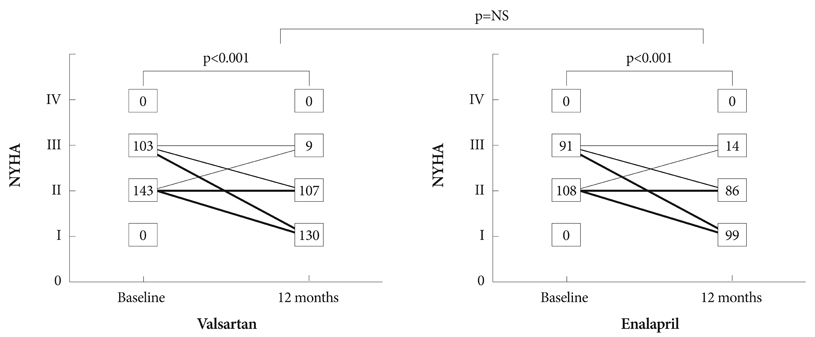
Fig. 2 Changes in NYHA functional class during treatment in the two groups. NYHA: New York Heart Association.

Fig. 3 Change of NT-pro-BNP and high sensitive C-reactive protein before and after treatment. NT-pro-BNP: N-terminal pro-brain natriuretic peptide, hs-CRP: high sensitive C-reactive protein.

Fig. 4 Change of NT-pro-BNP according to change of left ventricular ejection faction (LVEF) and LV end diastolic dimension (LVEDD). NT-pro-BNP: N-terminal pro-brain natriuretic peptide, hs-CRP: high sensitive C-reactive protein.
Reference
-
1. Harrap SB, Dominiczak AF, Fraser R, et al. Plasma angiotensin II, predisposition to hypertension, and left ventricular size in healthy young adults. Circulation. 1996. 93:1148–1154.2. Kasama S, Toyama T, Kumakura H, et al. Spironolactone improves cardiac sympathetic nerve activity and symptoms in patients with congestive heart failure. J Nucl Med. 2002. 43:1279–1285.3. Curtiss C, Cohn JN, Vrobel T, Franciosa JA. Role of the renin-angiotensin system in the systemic vasoconstriction of chronic congestive heart failure. Circulation. 1978. 58:763–770.4. The CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure. Results of the cooperative north Scandinavian enalapril survival study (CONSENSUS). N Engl J Med. 1987. 316:1429–1435.5. The SOLVD Investigators. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. N Engl J Med. 1991. 325:293–302.6. Cohn JN, Tognoni G. Valsartan Heart Failure Trial Investigators. A randomized trial of the angiotensin-receptor blocker valsartan in chronic heart failure. N Engl J Med. 2001. 345:1667–1675.7. Koglin J, Pehlivanli S, Schwaiblmair M, Vogeser M, Cremer P, von-Scheidt W. Role of brain natriuretic peptide in risk stratification of patients with congestive heart failure. J Am Coll Cardiol. 2001. 38:1934–1941.8. Kim SH, Kim JS, Baek KK, et al. Role of NT-proBNP in evaluation of functional status in congestive heart failure. Korean Circ J. 2004. 34:894–899.9. Yasue H, Yoshimura M, Sumida H, et al. Localization and mechanism of secretion of NT-pro-natriuretic peptide in comparison with those of A-type natriuretic peptide in normal subjects and patients with heart failure. Circulation. 1994. 90:195–203.10. Tsutamoto T, Wada A, Maeda K, et al. Attenuation of compensation of endogenous cardiac natriuretic peptide system in chronic heart failure: prognostic role of plasma brain natriuretic peptide concentration in pa-tients with chronic symptomatic left ventricular dysfunction. Circulation. 1997. 96:509–516.11. Lang RM, Bierig M, Devereux RB, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography's Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005. 18:1440–1463.12. McDonagh TA, Robb SD, Murdoch DR, et al. Biochemical detection of left-ventricular systolic dysfunction. Lancet. 1998. 351:9–13.13. Tsutamoto T, Wada A, Maeda K, et al. Plasma brain natriuretic peptide level as a biochemical marker of morbidity and mortality in patients with asymptomatic or minimally symptomatic left ventricular dysfunction. Eur Heart J. 1999. 20:1799–1807.14. Chung IH, Yoo BS, Ryu HY, et al. The relationship between the early follow-up BNP level and congestive status or prognosis in acute heart failure. Korean Circ J. 2006. 36:200–207.15. Maeda K, Tsutamoto T, Wada A, et al. High levels of plasma brain natriuretic peptide and interleukin-6 after optimized treatment for heart failure are independent risk factors for morbidity and mortality in patients with congestive heart failure. J Am Coll Cardiol. 2000. 36:1587–1593.16. Troughton RW, Frampton CM, Yandle TG, Espiner EA, Nicholls MG, Richards AM. Treatment of heart failure guided by plasma aminoterminal brain natriuretic peptide (N-BNP) concentrations. Lancet. 2000. 355:1126–1130.17. Nagaya N, Nishikimi T, Goto Y, et al. Plasma brain natriuretic peptide is a biochemical marker for the prediction of progressive ventricular remodeling after acute myocardial infarction. Am Heart J. 1998. 135:21–28.18. Latini R, Masson S, Anand I, et al. Effects of valsartan on circulating brain natriuretic peptide and norepinephrine in symptomatic chronic heart failure: the Valsartan Heart Failure Trial (Val-HeFT). Circulation. 2002. 106:2454–2458.19. Kasama S, Toyama T, Hatori T, et al. Comparative effects of valsartan and enalapril on cardiac sympathetic nerve activity and plasma brain natriuretic peptide in patients with congestive heart failure. Heart. 2006. 92:625–630.20. Kohno M, Horio T, Yokokawa K, et al. Brain natriuretic peptide as a cardiac hormone in essential hypertension. Am J Med. 1992. 92:29–34.21. Levin ER, Gardner DG, Samson WK. Natriuretic peptides. N Engl J Med. 1998. 339:321–328.22. Tseng DS, Kwong J, Rezvani F, Coates AO. Angiotensin-converting enzyme-related cough among Chinese-Americans. Am J Med. 2010. 123:183.e11–183.e15.23. Woo KS, Norris RM, Nicholls G. Racial differences in incidence of cough with angiotensin-converting enzyme inhibitors (a tale of two cities). Am J Cardiol. 1995. 75:967–968.24. Nishizawa A. Angiotensin-converting enzyme inhibitor induced cough among Asians. Proc UCLA Health. 2000. 4:35–38.25. Yeo WW, Ramsay LE. Persistent dry cough with enalapril: incidence depends on the method used. J Hum Hypertens. 1990. 4:517–520.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Biomarkers in Heart Failure: Focus on B-type Natriuretic Peptide
- Clinical Implication of B-type Natriuretic Peptide in the Elderly
- Changes in N-terminal pro-B-type natriuretic peptide in a neonate with symptomatic isolated left ventricular noncompaction
- Serial Monitoring of B-Type Natriuretic Peptide in Heart Failure Patients
- Prediction of Outcome in Subarachnoid Hemorrhage with N-terminal Probrain Natriuretic Peptide (NT-proBNP)
