Serial Monitoring of B-Type Natriuretic Peptide in Heart Failure Patients
- Affiliations
-
- 1Department of Cardiology, Wonju College of Medicine, Yonsei University, Wonju, Korea. yubs@yonsei.ac.kr
- KMID: 2093974
- DOI: http://doi.org/10.4070/kcj.2007.37.9.393
Abstract
- The measurements of B-type natriuretic peptide (BNP) or N-terminal proBNP (NT-proBNP), when taken together with conventional clinical assessment, may assist in making the prognosis and also for making serial adjustment of such treatment. But although such commercial assays are currently approved for the diagnosis of heart failure, the role of the natriuretic peptides for monitoring the success of congestive heart failure (CHF) therapy has not as yet been submitted for regulatory approval. Moreover, because of the intra-individual biologic variation of the BNP or because of multiple factors that affect the BNP levels, the magnitude of the change of BNP levels must be large to confidently interpret BNP changes within an individual, and just how large has not been determined. Yet the levels of plasma BNP and NT-pro BNP are well correlated with the concurrent haemodynamic measurements and indicators of left ventricular systolic function. Also, BNP and NT-pro BNP serve as significant prognostic information and it is possible that adjustment of anti-heart failure therapy according to serial measurements of BNP (in addition to the standard clinical assessment) may offer improved outcomes. Better understanding of the test characteristics is needed before we can effectively use this valuable test to guide therapeutic strategies.
MeSH Terms
Figure
-
Fig. 1 Diagram of the potential roles of B-type natriuretic peptide (BNP) or N-terminal proBNP (NT-proBNP). Testing for either BNP or NT-proBNP has a number of possible uses for the treatment of heart failure: screening for asymptomatic left ventricular dysfunction, diagnosis, risk stratification, determining the prognosis and treatment monitoring.

Fig. 2 Neuro-hormone imbalance in heart failure. For patients with heart failure, the rennin-angiotensin-aldosterone system, the sympathetic nerve system and the endothelin systems are activated over the counter-regulatory natriuretic peptide (BNP, ANP) systems or other systems (A). Therefore, neurohormonal imbalance is a significant patho-physiologic mechanism in heart failure. After treatment, recovery of the neurohormonal balance means stabilization of the heart failure status (B). BNP: B-type natriuretic peptide, ANP: A-type natriuretic peptide, RAS: renin-angiotensin-aldosterone system, SNS: sympathetic nervous system.
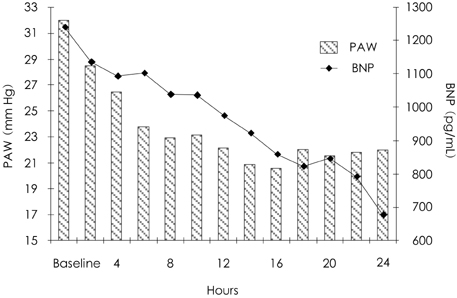
Fig. 3 Relationship of the B-type natriuretic peptide (BNP) levels and the pulmonary wedge pressure (PAW) in patients with heart failure.14) During 24 hours of treatment for patient with decompensated congestive heart failure, the wedge pressure decreased below 20 mm Hg within 16 hours and then remained there. As the wedge pressure fell, so did the BNP level. It is interesting to note that even after the wedge pressures normalized in these patients, the BNP levels continued to decline. This reflects continual neuro-hormonal normalization and the BNP was a relatively good indicator for treatment monitoring.

Fig. 4 Percent reduction in the N-terminal proBNP (NT-proBNP) levels according to the clinical course during hospitalization.8) The NT-proBNP levels were significantly lower in patients with complete resolution than those in the patients with an insufficient response to therapy (p<0.05). BNP: B-type natriuretic peptide.
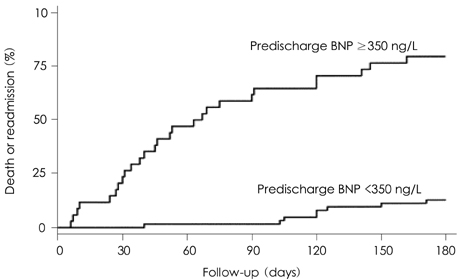
Fig. 5 Kaplan-Meier curves according to the predefined B-type natriuretic peptide (BNP) cut off (350 ng/L).9) Predischarge BNP levels >350 ng/L are strongly related to death or re-admission (HR=12.6 [5.7 to 28.1], p=0.0001), and the rate of events reached 23.5% at one month and 79.4% at six months.
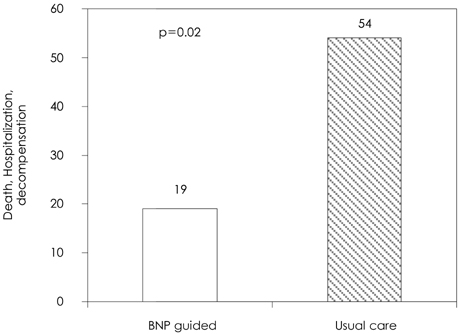
Fig. 6 Outcomes and treatment of heart failure as guided by N-terminal proBNP (NT-proBNP).19) This figure shows a significant reduction in events in that group whose treatment was adjusted according to serial measurements of plasma NT-proBNP. BNP: B-type natriuretic peptide.
Cited by 1 articles
-
Preliminary Clinical Experience with Waon Therapy in Korea: Safety and Effect
Il-Suk Sohn, Jin-Man Cho, Woo-Shik Kim, Chong-Jin Kim, Kwon-Sam Kim, Jong-Hoa Bae, Chuwa Tei
J Cardiovasc Ultrasound. 2010;18(2):37-42. doi: 10.4250/jcu.2010.18.2.37.
Reference
-
1. Tsutamoto T, Wada A, Maeda K, et al. Attenuation of compensation of endogenous cardiac natriuretic peptide system in chronic heart failure: prognostic role of plasma brain natriuretic peptide concentration in patients with chronic symptomatic left ventricular dysfunction. Circulation. 1997. 96:509–516.2. Cowie MR, Struthers AD, Wood DA, et al. Value of natriuretic peptides in assessment of patients with possible new heart failure in primary care. Lancet. 1997. 350:1349–1353.3. Dao Q, Krishnaswamy P, Kazanegra R, et al. Utility of B-type natriuretic peptide in the diagnosis of congestive heart failure in an urgent-care setting. J Am Coll Cardiol. 2001. 37:379–385.4. Maisel AS, Krishnaswamy P, Nowak RM, et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med. 2002. 347:161–167.5. Maisel AS. The diagnosis of acute congestive heart failure: role of BNP measurements. Heart Fail Rev. 2003. 8:327–334.6. Maisel AS, McCord J, Nowak RM, et al. Bedside B-Type natriuretic peptide in the emergency diagnosis of heart failure with reduced or preserved ejection fraction. J Am Coll Cardiol. 2003. 41:2010–2017.7. Yoo BS, Kim WJ, Jung HS, et al. The clinical experiences of B-type natriuretic peptide blood concentrations for diagnosis in congestive heart failure: the single hospital experience based on the large clinical database. Korean Circ J. 2004. 34:684–692.8. Bayes-Genis A, Santalo-Bel M, Zapico-Muniz E, et al. N-terminal probrain natriuretic peptide (NT-proBNP) in the emergency diagnosis and in-hospital monitoring of patients with dyspnoea and ventricular dysfunction. Eur J Heart Fail. 2004. 6:301–308.9. Logeart D, Thabut G, Jourdain P, et al. Predischarge B-type natriuretic peptide assay for identifying patients at high risk of re-admission after decompensated heart failure. J Am Coll Cardiol. 2004. 43:635–641.10. Anand IS, Fisher LD, Chiang YT, et al. Changes in brain natriuretic peptide and norepinephrine over time and mortality and morbidity in the Valsartan Heart Failure Trial (Val-HeFT). Circulation. 2003. 107:1278–1283.11. Chung IH, Yoo BS, Ryu HY, et al. The relationship between the early follow-up BNP level and congestive status or prognosis in acute heart failure. Korean Circ J. 2006. 36:200–207.12. Stevenson LW, Perloff JK. The limited reliability of physical signs for estimating hemodynamics in chronic heart failure. JAMA. 1989. 261:884–888.13. Mahdyoon H, Klein R, Eyler W, Lakier JB, Chakko SC, Gheorghiade M. Radiographic pulmonary congestion in end-stage congestive heart failure. Am J Cardiol. 1989. 63:625–627.14. Kazanegra R, Cheng V, Garcia A, et al. A rapid test for B-type natriuretic peptide correlates with falling wedge pressures in patients treated for decompensated heart failure: a pilot study. J Card Fail. 2001. 7:21–29.15. Cheng V, Kazanagra R, Garcia A, et al. A rapid bedside test for B-type peptide predicts treatment outcomes in patients admitted for decompensated heart failure: a pilot study. J Am Coll Cardiol. 2001. 37:386–391.16. Tang WH, Girod JP, Lee MJ, et al. Plasma B-type natriuretic peptide levels in ambulatory patients with established chronic symptomatic systolic heart failure. Circulation. 2003. 108:2964–2966.17. Richards AM, Crozier IG, Yandle TG, Espiner EA, Ikram H, Nicholls MG. Brain natriuretic factor: regional plasma concentrations and correlations with haemodynamic state in cardiac disease. Br Heart J. 1993. 69:414–417.18. Murdoch DR, McDonagh TA, Byrne J, et al. Titration of vasodilator therapy in chronic heart failure according to plasma brain natriuretic peptide concentration: randomized comparison of the hemodynamic and neuroendocrine effects of tailored versus empirical therapy. Am Heart J. 1999. 138:1126–1132.19. Troughton RW, Frampton CM, Yandle TG, Espiner EA, Nicholls MG, Richards AM. Treatment of heart failure guided by plasma aminoterminal brain natriuretic peptide (N-BNP) concentrations. Lancet. 2000. 355:1126–1130.20. Jourdain P, Jondeau G, Funck F, et al. Plasma brain natriuretic peptide-guided therapy to improve outcome in heart failure. J Am Coll Cardiol. 2007. 49:1733–1739.21. Haug C, Metzele A, Steffgen J, Kochs M, Hombach V, Grunert A. Increased brain natriuretic peptide and atrial natriuretic peptide plasma concentrations in dialysis-dependent chronic renal failure and in patients with elevated left ventricular filling pressure. Clin Investig. 1994. 72:430–434.22. Wang HS, Yoo BS, Chung IH, et al. Is B-type natriuretic peptide (BNP) measurement useful test for diagnosing systolic heart failure in patients with moderate to severe renal insufficiency? Korean Circ J. 2005. 35:897–903.23. Wu AH, Smith A, Wieczorek S, et al. Biological variation for N-terminal pro- and B-type natriuretic peptides and implications for therapeutic monitoring of patients with congestive heart failure. Am J Cardiol. 2003. 92:628–631.24. Wu AH, Smith A. Biological variation of the natriuretic peptides and their role in monitoring patients with heart failure. Eur J Heart Fail. 2004. 6:355–358.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Biomarkers in Heart Failure: Focus on B-type Natriuretic Peptide
- Clinical Implication of B-type Natriuretic Peptide in the Elderly
- High Plasma Levels of the B-type Natriuretic Peptide in Patients Without Heart Failure: Is There Clinical Significance?
- The Role of Brain Natriuretic Peptide in the Patients with Acute Dyspnea in the Emergency Department
- Bio-Molecular Markers for Cardiovascular Disease: Significance of Natriuretic Peptides and Adrenomedullin
