J Rheum Dis.
2014 Feb;21(1):30-34. 10.4078/jrd.2014.21.1.30.
A Case of Sclerosing Encapsulating Peritonitis Presented with Systemic Lupus Erythematosus
- Affiliations
-
- 1Department of Internal Medicine, Inje University Ilsan Paik Hospital, Goyang, Korea. byyoon@paik.ac.kr
- 2Department of Internal Medicine, Inje Univeristy Seoul Paik Hospital, Seoul, Korea.
- KMID: 2222986
- DOI: http://doi.org/10.4078/jrd.2014.21.1.30
Abstract
- Sclerosing encapsulating peritonitis (SEP) is characterized by peritoneal fibrosis and adhesion of the peritoneum with the loops of the small intestine. Although the prevalence is low, most cases are caused by peritoneal dialysis, infection, medication, systemic lupus erythematosus (SLE), and intra-abdominal neoplasm. We describe a 22-year old man who was presented with abdominal pain and distension, which were attributed to SLE with peritonitis. He had no specific history of previous medical illness and peritoneal dialysis. He was treated with intravenous high dose methylprednisolone 1 g/day for 3 days, followed by intravenous methylprednisolone 1 mg/kg daily and immunoglobulin. However, his symptoms did not improve. Eventually, a laparoscopic biopsy was performed for an accurate diagnosis. The histopathologic findings were presented in accordance to the typical characteristics of SEP. In spite of medical treatment, he did not show an improvement of clinical symptoms and radiologic findings. As a result, he died from nutritional deficiency, upper gastrointestinal bleeding, and congestive heart failure.
MeSH Terms
Figure
-
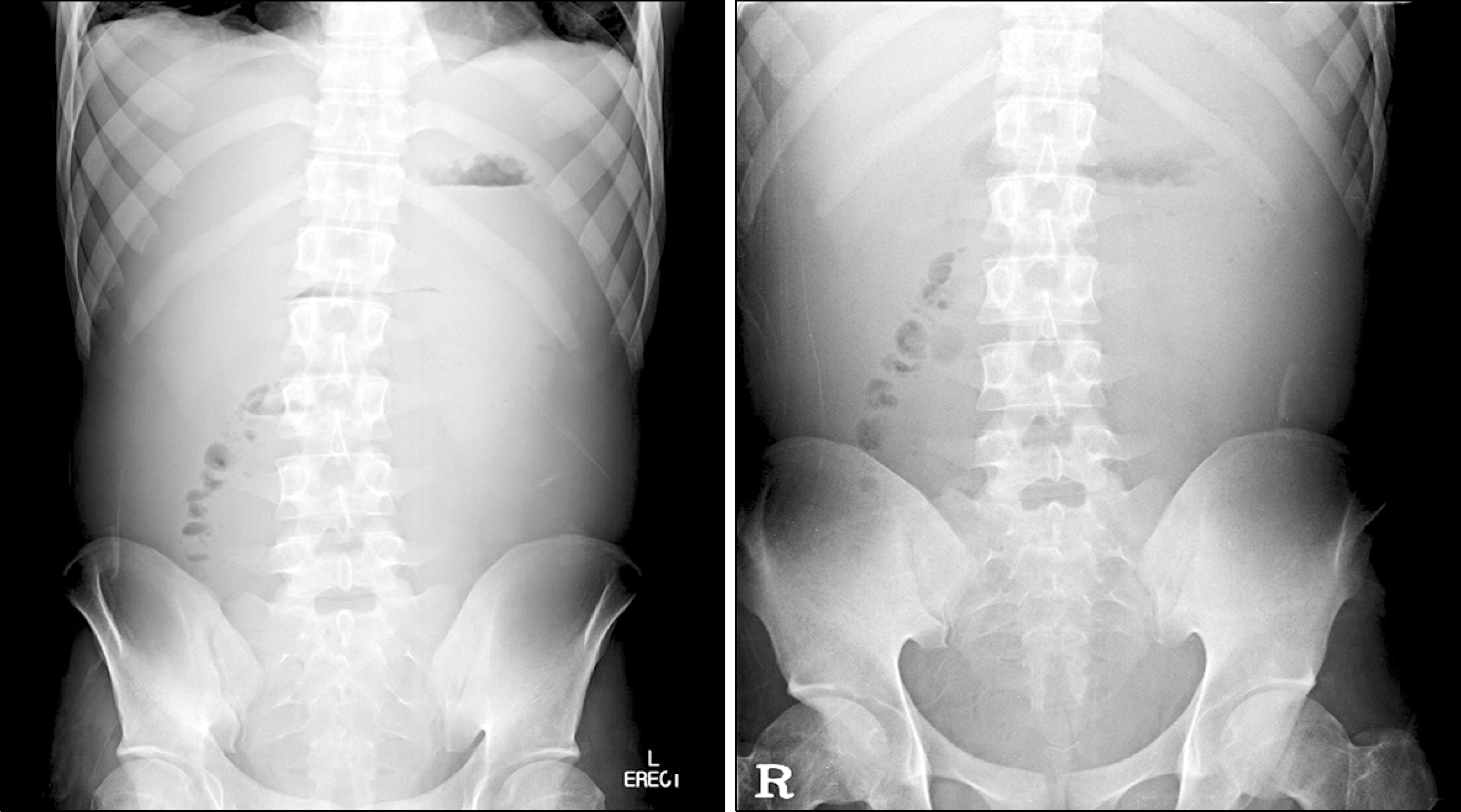
Figure 1. Simple abdomen erect and supine on admission showed centralization of bowel loop, sug-gesting large amount of ascites.

Figure 2. Abdominal pelvic CT on admission showed small bowel diffuse wall thickening and centralization with marked ascites (A). On day 21 of therapy, Followup CT scan showed no remarkable changes (B).
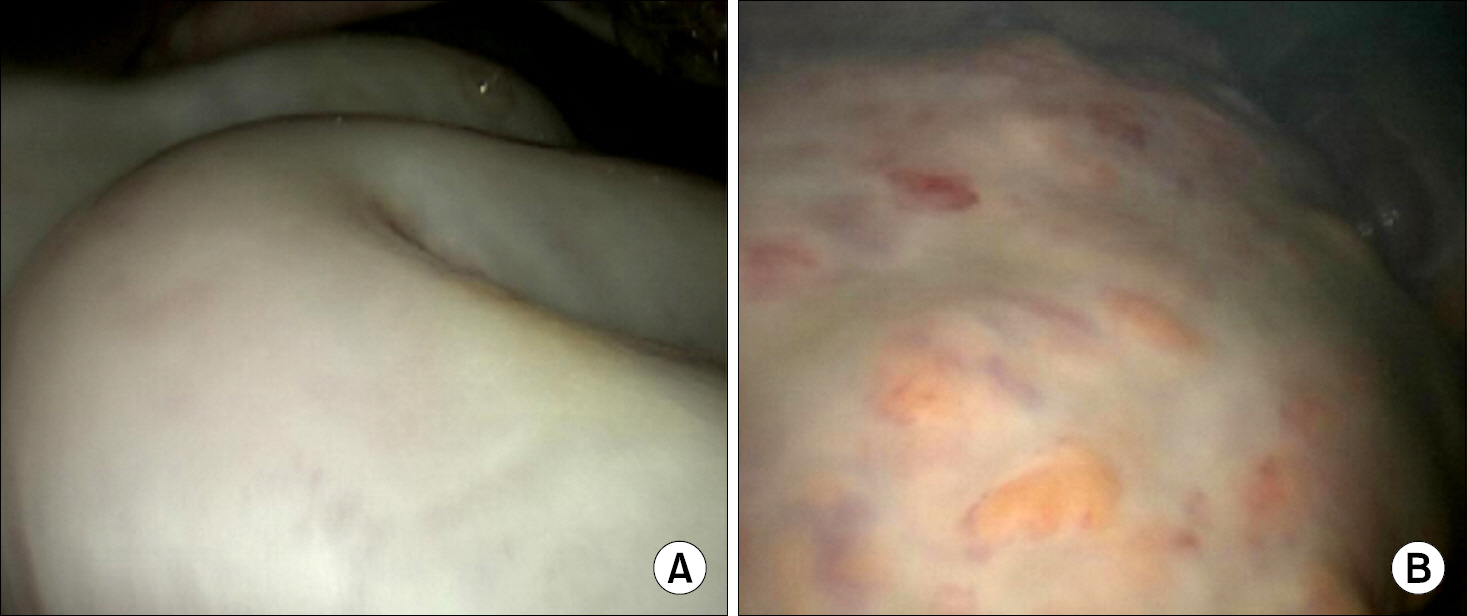
Figure 3. The peritoneum (A) and greater omentum (B) showed fibrotic change and, fibrotic peritoneum covered small intestine at laparo-tomy.
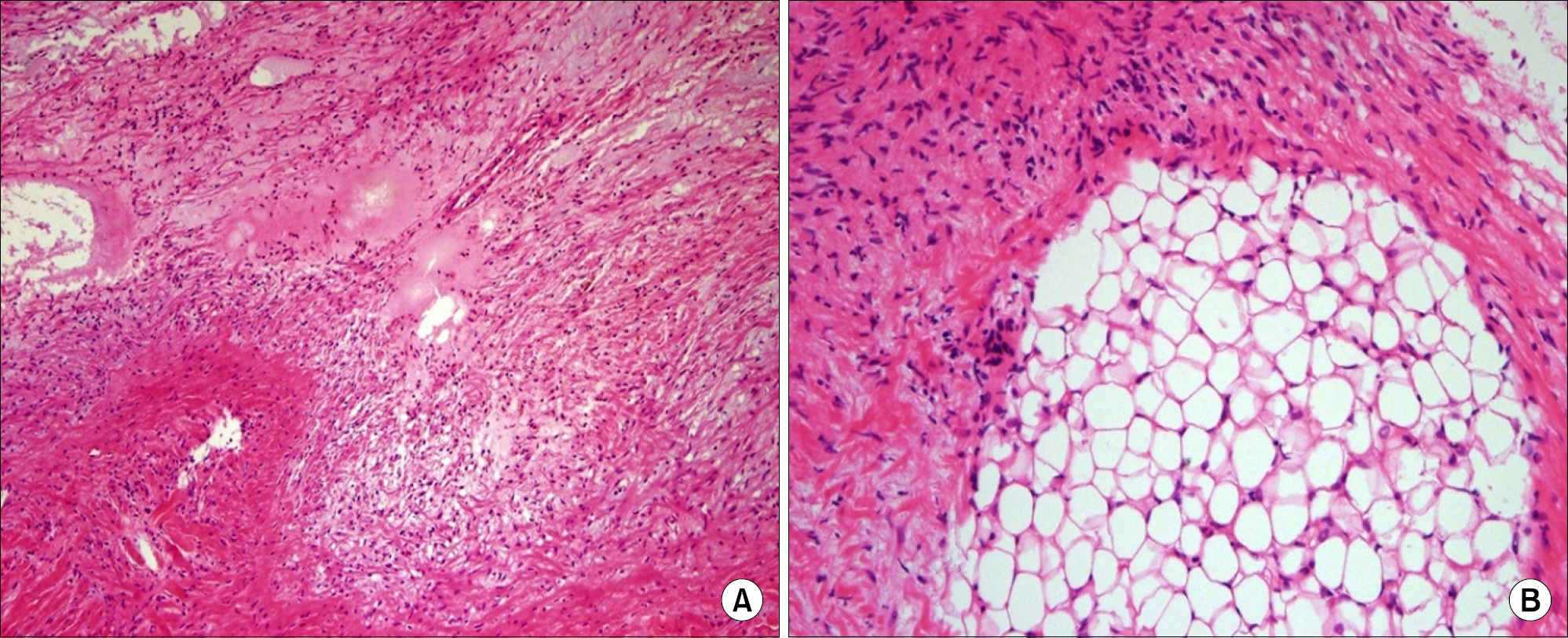
Figure 4. Histopathology in peritoneum (A, H&E stain, ×100) and greater omentum (B, H&E stain, ×200) showed fibrosis and fibroblast hyperproliferation accompanying lymphocyte infiltration.
Reference
-
References
1. Eltoum MA, Wright S, Atchley J, Mason JC. Four con- secutive cases of peritoneal dialysis-related encapsulating peritoneal sclerosis treated successfully with tamoxifen. Perit Dial Int. 2006; 26:203–6.2. Kawanishi H, Moriishi M. Epidemiology of encapsulating peritoneal sclerosis in Japan. Perit Dial Int. 2005; 25(Suppl 4):S14–8.
Article3. Kobayashi TK, Ueda M, Nishino T, Nishida S, Yoneyama C, Watanabe S. Appearance of "collagen balls" in ascitic fluid cytology with abdominal cocoon (encapsulating peritonitis) Diagn Cytopathol. 1997; 16:469–70.4. Odama UO, Shih DJ, Korbet SM. Sclerosing peritonitis and systemic lupus erythematosus: a report of two cases. Perit Dial Int. 1999; 19:160–4.
Article5. Pepels MJ, Peters FP, Mebis JJ, Ceelen TL, Hoofwijk AG, Erdkamp FL. Sclerosing peritonitis: an unusual cause of ascites in a patient with systemic lupus erythematosus. Neth J Med. 2006; 64:346–9.6. Garosi G, Di Paolo N. Peritoneal sclerosis: one or two nosological entities? Semin Dial. 2000; 13:297–308.7. Burstein M, Galun E, Ben-Chetrit E. Idiopathic sclerosing peritonitis in a man. J Clin Gastroenterol. 1990; 12:698–701.
Article8. Cleffken B, Sie G, Riedl R, Heineman E. Idiopathic sclerosing encapsulating peritonitis in a young female-diagnosis of abdominal cocoon. J Pediatr Surg. 2008; 43:e27–30.
Article9. Pott Júnior H, Amate Neto A, Teixeira MA, Provenza JR. Ascites due to lupus peritonitis: a rare form of onset of systemic lupus erythematosus. Rev Bras Reumatol. 2012; 52:116–9.10. Masuda C, Fujii Y, Kamiya T, Miyamoto M, Nakahara K, Hattori S, et al. Idiopathic sclerosing peritonitis in a man. Intern Med. 1993; 32:552–5.
Article11. Bansal S, Sheth H, Siddiqui N, Bender FH, Johnston JR, Piraino B. Incidence of encapsulating peritoneal sclerosis at a single U.S. university center. Adv Perit Dial. 2010; 26:75–81.12. Sampimon DE, Kolesnyk I, Korte MR, Fieren MW, Struijk DG, Krediet RT. Use of angiotensin II inhibitors in patients that develop encapsulating peritoneal sclerosis. Perit Dial Int. 2010; 30:656–9.
Article13. Kawanishi H, Kawaguchi Y, Fukui H, Hara S, Imada A, Kubo H, et al. Encapsulating peritoneal sclerosis in Japan: a prospective, controlled, multicenter study. Am J Kidney Dis. 2004; 44:729–37.
Article14. Ryu HJ, Park YB, Lee JH, Lee HS, Lee EY, Lee YJ, et al. A case of idiopathic sclerosing peritonitis. J Korean Rheum Assoc. 2008; 15:180–5.
Article15. Jung JY, Jang WI, Yoon JH, Kim ES, Chung S, Choi DE, et al. Successful treatment of Sclerosing encapsulating peritonitis with tamoxifen and prednisolone. Korean J Nephrol. 2009; 28:685–92.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Sclerosing Encapsulating Peritonitis in Chronic Ambulatory Peritoneal Dialysis; Preoperative Catheter Drainage: A Case Report
- A Case of Transverse Myelitis as a First Manifestation of Systemic Lupus Erythematosus
- A Ruptured Aneurysm in a Patient with Systemic Lupus Erythematosus: Case Report
- A Case Of Systemic Lupus Erythematosus Associated With Hyperthyroidism And Severe Retinopathy
- A Case of Systemic Lupus Erythematosus with Initial Clinical Presentation of Peritonitis
