Postural Intraocular Pressure Change at Trendelenberg Position Measured by Rebound Tonometer
- Affiliations
-
- 1Department of Ophthalmology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea. kihopark@snu.ac.kr
- 2Department of Medicine, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2218418
- DOI: http://doi.org/10.3341/jkos.2014.55.2.247
Abstract
- PURPOSE
This study was carried out to evaluate the postural intraocular pressure (IOP) change in Trendelenburg, reverse Trendelenburg, and supine positions in healthy young males.
METHODS
We measured the IOP values of 5 healthy young male volunteers (10 eyes) using an Icare PRO rebound tonometer in sitting, Trendelenburg, reverse Trendelenburg, and supine positions.
RESULTS
The mean IOP in the supine position (18.63 mm Hg) was significantly higher (p < 0.01) than in the sitting position (15.31 mm Hg). When maintaining the Trendelenburg position, IOP gradually increased.
CONCLUSIONS
In our study, the Trendelenburg position significantly increased the IOP compared to that in the supine position. The effects of increased IOP should be considered in situations that require Trendelenburg positioning, such as exercise or surgery.
Keyword
MeSH Terms
Figure
-
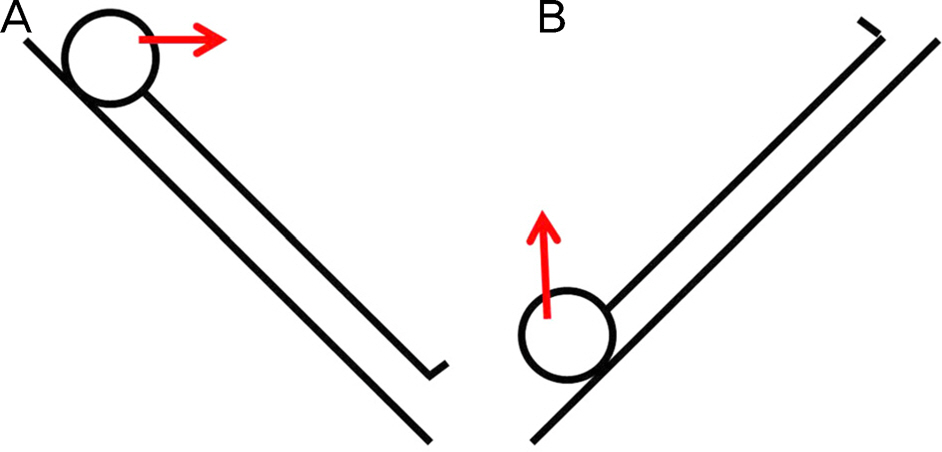
Figure 1. Illustration of experimental positions. Reverse Trend- enlenburg position (T3, 4, 5, 6) (A) and Trendelenburg pos-iton (T8, 9, 10) (B). Red arrow indicates the direction of patient's eyes.
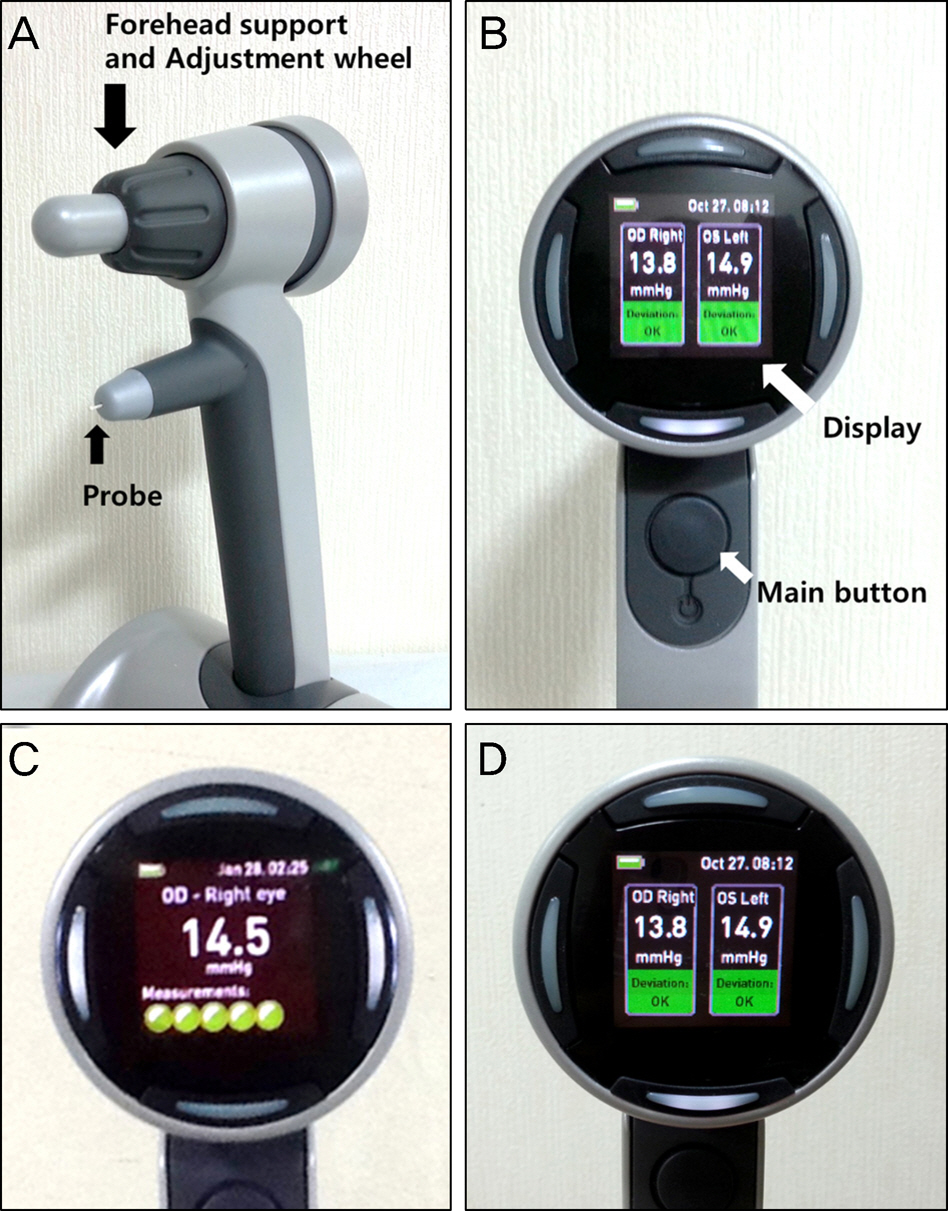
Figure 2. Icare PRO rebound tonometer (Icare® PRO; Icare Finland Oy, Helsinki, Finland) Front view (A) and rear view (B) of Icare PRO, (C) display during measuring IOP, (D) display after measuring IOP, showing reliability below IOP. IOP = intraocular pressure.
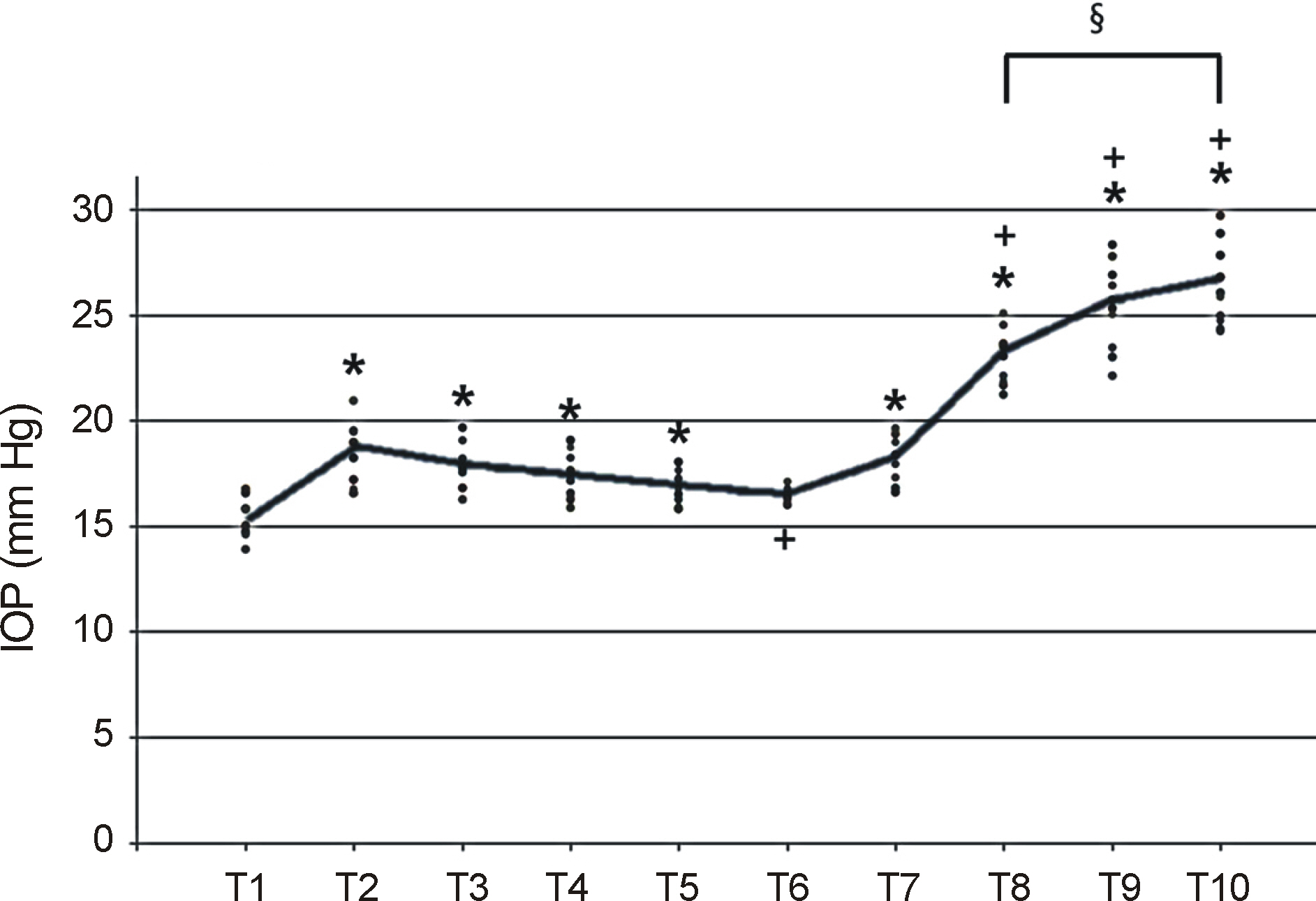
Figure 3. Scatter plot of the IOP with the overlaid line con-necting the mean IOP at each time point. IOP = intraocular pressure; T1 = Sitting; T2 = 10 minutes after supine position; T3 = 10 minutes after reverse Trendelenburg position; T4 = 20 minutes after reverse Trendelenburg position; T5 = 30 minutes after reverse Trendelenburg position; T6 = 60 minutes after reverse Trendelenburg position; T7 = 10 minutes after supine position; T8 = 10 minutes after Trendelenburg position; T9 = 20 minutes after Trendelenburg position; T10 = 30 minutes after Trendelenburg position. * Indicates significant difference compared to T1 (p < 0.05, Tahame’s test). † Indicates significant difference compared to T2 (p < 0.05, Tahame’s test). ‡Indicates significant difference between T8 and T10 (p < 0.05, Tahame’s test).
Reference
-
References
1. Heijl A, Leske MC, Bengtsson B. et al. Early Manifest Glaucoma Trial Group. Reduction of intraocular pressure and glaucoma pro-gression: results from the Early Manifest Glaucoma Trial. Arch Ophthalmol. 2002; 120:1268–79.2. Kass MA, Heuer DK, Higginbotham EJ. . The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002; 120:701–13. dis-cussion 829-30.3. Lee JY, Yoo C, Jung JH. . The effect of lateral decubitus posi-tion on intraocular pressure in healthy young subjects. Acta Ophthalmol. 2012; 90:e68–72.
Article4. Lee JY, Yoo C, Kim YY.The effect of lateral decubitus position on intraocular pressure in patients with untreated open-angle glaucoma. Am J Ophthalmol. 2013; 155:329–35.e2.
Article5. Tsukahara S, Sasaki T.Postural change of IOP in normal persons and in patients with primary wide open-angle glaucoma and low-tension glaucoma. Br J Ophthalmol. 1984; 68:389–92.
Article6. Carlson KH, McLaren JW, Topper JE, Brubaker RF.Effect of body position on intraocular pressure and aqueous flow. Invest Ophthalmol Vis Sci. 1987; 28:1346–52.7. Gartner S, Beck W.Ocular tension in the trendelenburg position. Am J Ophthalmol. 1965; 59:1040–3.8. Lee K, Lee JY, Moon JI, Park MH.Comparison of icare rebound tonometer with goldmann applanation tonometry. J Korean Ophthalmol Soc. 2013; 54:296–302.
Article9. Lee JS, Kim CM, Choi HY, Oum BS.A relationship between intra-ocular pressure and age and body mass index in a Korean population. J Korean Ophthalmol Soc. 2003; 44:1559–66.10. Anderson DR, Grant WM.The influence of position on intraocular pressure. Invest Ophthalmol. 1973; 12:204–12.11. Martinez-de-la-Casa JM, Garcia-Feijoo J, Castillo A, Garcia-Sanchez J.Reproducibility and clinical evaluation of rebound tonometry. Invest Ophthalmol Vis Sci. 2005; 46:4578–80.
Article12. Awad H, Santilli S, Ohr M. . The effects of steep trendelenburg positioning on intraocular pressure during robotic radical pros- tatectomy. Anesth Analg. 2009; 109:473–8.13. Weber ED, Colyer MH, Lesser RL, Subramanian PS.Posterior is-chemic optic neuropathy after minimally invasive prostatectomy. J Neuroophthalmol. 2007; 27:285–7.
Article14. Moraine JJ, Berré J, Mélot C.Is cerebral perfusion pressure a major determinant of cerebral blood flow during head elevation in coma-tose patients with severe intracranial lesions? J Neurosurg. 2000; 92:606–14.
Article15. Nardi M, Bartolomei MP, Romani A, Barca L.Intraocular pressure changes in secondary positions of gaze in normal subjects and in restrictive ocular motility disorders. Graefes Arch Clin Exp Ophthalmol. 1988; 226:8–10.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Intraocular Pressures According to Position Using Icare Rebound Tonometer
- Reliability Comparison of Rebound Tonometer at the Upright and Supine Position
- Intraocular Pressure Measurement with the Noncontact Tonometer and Rebound Tonometer through Plano Soft Contact Lenses
- Comparison of Portable Tonometers and Goldmann Applanation Tonometer for Intraocular Pressure Measurement
- Clinical Comparision of the ProTon and the Goldmann Applanation Tonometer
