Analysis of Clinical Characteristics in Phlyctenular Keratoconjunctivitis at a Tertiary Center
- Affiliations
-
- 1Department of Ophthalmology, Seoul National University College of Medicine, Seoul, Korea. kmk9@snu.ac.kr
- 2Seoul Artificial Eye Center, Seoul National University Hospital Clinical Research Institute, Seoul, Korea.
- 3Department of Ophthalmology, Seoul National University Bundang Hospital, Seongnam, Korea.
- KMID: 2214131
- DOI: http://doi.org/10.3341/jkos.2011.52.1.7
Abstract
- PURPOSE
To report the clinical characteristics of patients with phlyctenular keratoconjunctivitis at a tertiary care center in Korea.
METHODS
The authors of the present study retrospectively reviewed the medical records of 26 patients who were diagnosed with phlyctenular keratoconjunctivitis, identifying the age and sex at diagnosis, diagnosis of the referring clinic, laterality and location of the lesions, the results of bacterial cultures from the meibum, and treatment options.
RESULTS
Eighteen patients (76.2%) were female, and the mean age at diagnosis was 18.4 +/- 10.5 years. Nine patients (34.6%) showed evidence of bilateral diseases, and corneal lesions were observed in 27 eyes of 21 patients. Bacterial cultures from the meibum were performed for 17 patients, with the following results: 6 cases of Staphylococcus epidermidis, 4 cases of Corynebacterium species, and 1 case of Propionibacterium acne. Neovascularization with corneal phlyctenules occurred from the inferior quadrant mostly. Twenty-four patients received the remission treatment of prednisolone acetate 1% eye drops and evidence of regression of new vessels was observed in all patients. Three patients (16.7%) experienced recurrence despite the maintenance treatment of cyclosporine 0.05% eye drops. Visual acuities improved significantly after the remission treatment, as compared to the initial visit.
CONCLUSIONS
The phlyctenular keratoconjunctivitis patients who visited the tertiary center in Korea showed similar findings regarding demographics, involvement of blepharitis, and identified microorganisms, as compared with patients in previous reports. However, corneal lesions involving the visual axis were frequent, suggesting that with proper diagnosis and treatment, improvement in visual acuities is possible.
MeSH Terms
-
Acne Vulgaris
Blepharitis
Cornea
Corynebacterium
Cyclosporine
Demography
Eye
Female
Humans
Keratoconjunctivitis
Korea
Medical Records
Ophthalmic Solutions
Prednisolone
Propionibacterium
Recurrence
Retrospective Studies
Staphylococcus epidermidis
Tertiary Care Centers
Visual Acuity
Cyclosporine
Ophthalmic Solutions
Prednisolone
Figure
-
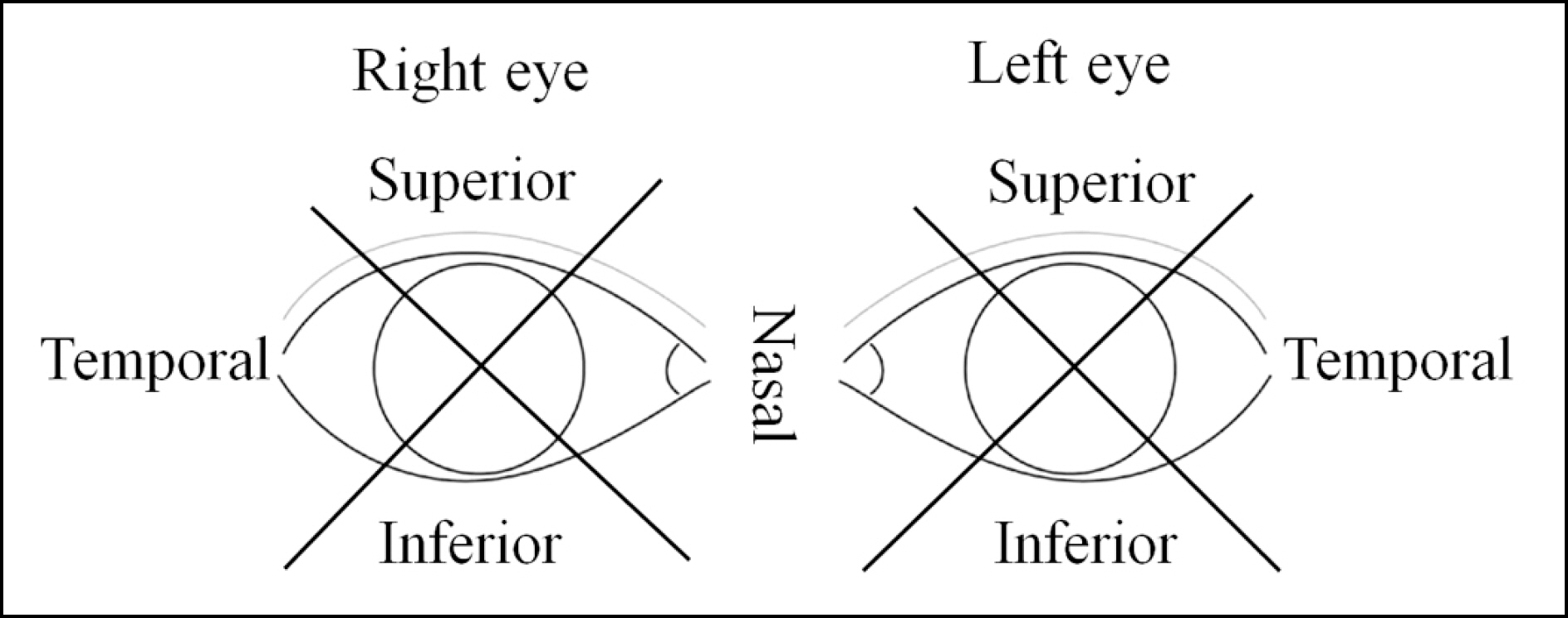
Figure 1. Diagram for definition of quadrant in analysis of involvement of phlyctenular keratitis.

Figure 2. Age distributions of phlyctenular keratoconjunctivitis patients: 5 patients under age 10, 13 patients between 11 and 20, 6 patients between 21 and 30, and 2 patients over age 31, 40 and 50, respectively.
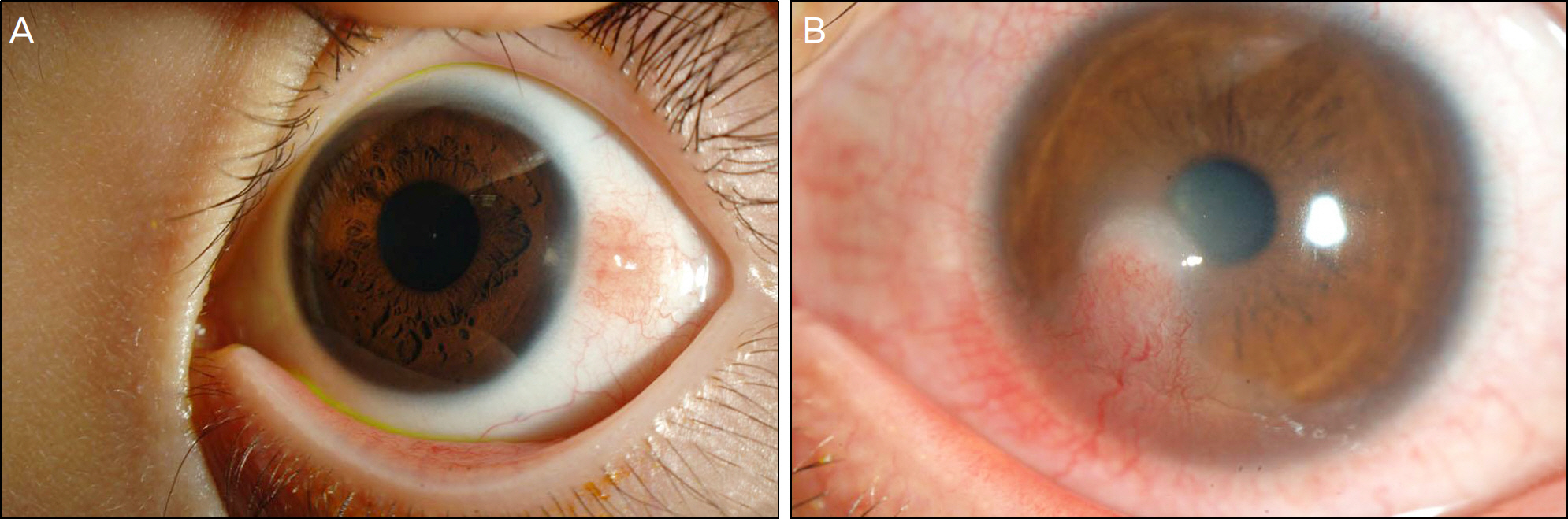
Figure 3. Representative cases of phlyctenular conjunctivitis (A) and keratitis (B). A whitish elevated lesion with neovascularization from the conjunctiva across the limbus was a typical manifestation of phlyctenular keratitis (B).
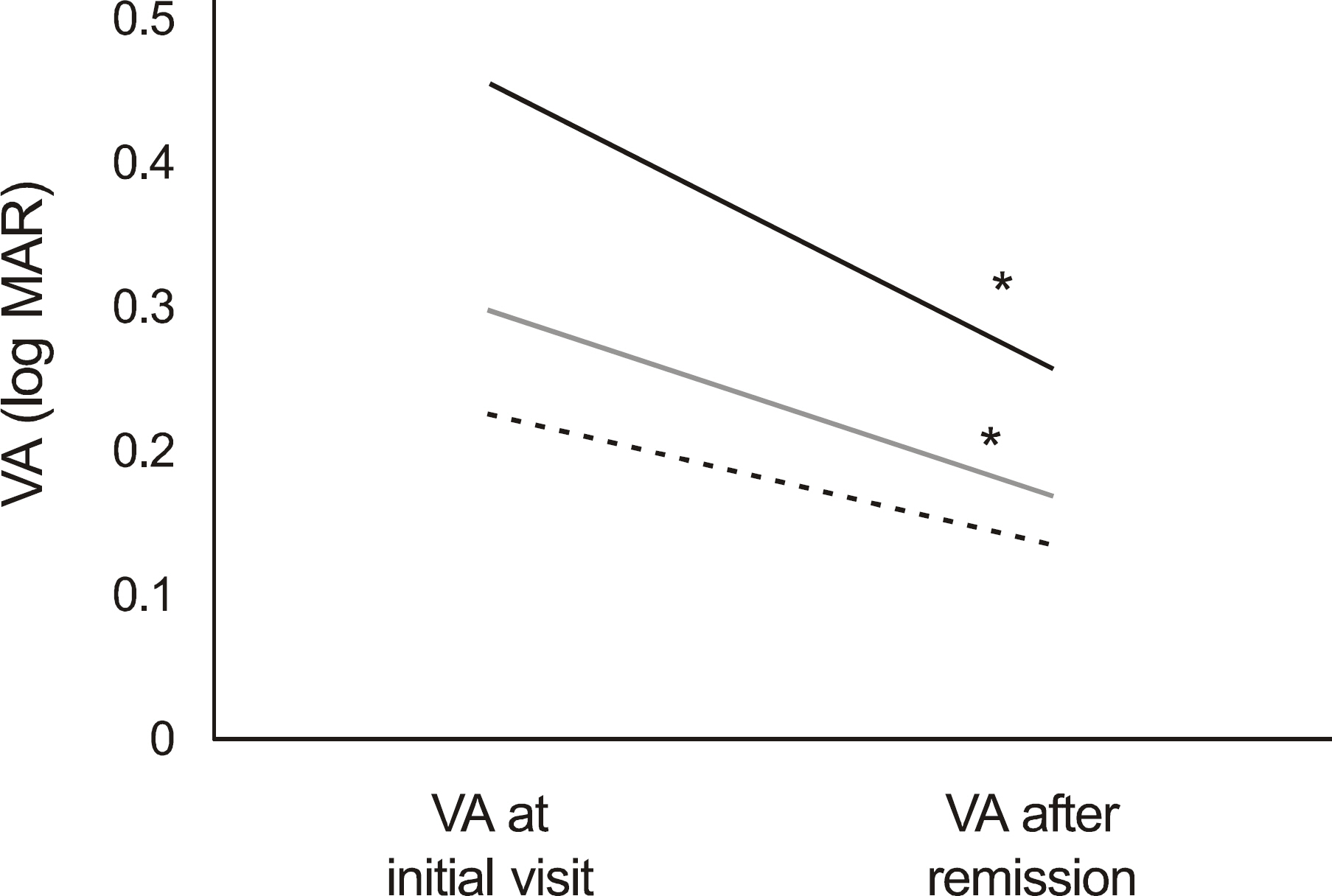
Figure 4. Visual acuity of phlyctenular keratitis patients. Visual acuity improved significantly after remission treatment in patients whose visual axes were threatened (P=0.028). Black line: Patients whose visual axes were threatened, gray line: All keratitis patients; dashed line: Patients whose visual axes were spared, asterisk (*): statistically significant (P<0.05).
Cited by 2 articles
-
Clinical Aspects of Phlyctenular Keratoconjunctivitis Using a Tear Film Interferometer
Dong Hyun Kang, Sang Wroul Song, Byung Yeop Kim, Kyu Yeon Hwang, Kook Young Kim
J Korean Ophthalmol Soc. 2020;61(1):1-8. doi: 10.3341/jkos.2020.61.1.1.Corneal Perforation in Phlyctenular Keratitis
Yong Sun Ahn, Jin A Lee, Yang Kyung Cho
J Korean Ophthalmol Soc. 2014;55(2):298-303. doi: 10.3341/jkos.2014.55.2.298.
Reference
-
References
1. Abu el Asrar AM, Geboes K, Maudgal PC, et al. Immunocytological study of phlyctenular eye disease. Int Ophthalmol. 1987; 10:33–9.
Article2. Singal A, Aggarwal P, Pandhi D, et al. Cutaneous tuberculosis and phlyctenular keratoconjunctivitis: a forgotten association. Indian J Dermatol Venereol Leprol. 2006; 72:290–2.
Article3. Ostler HB. Corneal perforation in nontuberculous (staphylococcal) phlyctenular keratoconjunctivitis. Am J Ophthalmol. 1975; 79:446–8.
Article4. Neiberg MN, Sowka J. Phlyctenular keratoconjunctivitis in a patient with Staphylococcal blepharitis and ocular rosacea. Optometry. 2008; 79:133–7.
Article5. Thygeson P. Observations on nontuberculous phlyctenular aberrations. Trans Am Acad Ophthalmol Otolaryngol. 1954; 58:128–32.6. Hird RB. Phlyctenular disease and its relation to tuberculosis. Br J Ophthalmol. 1918; 2:215–23.
Article7. Beauchamp GR, Gillette TE, Friendly DS. Phlyctenular aberrations. J Pediatr Ophthalmol Strabismus. 1981; 18:22–8.8. Suzuki T, Mitsuishi Y, Sano Y, et al. Phlyctenular keratitis associated with meibomitis in young patients. Am J Ophthalmol. 2005; 140:77–82.
Article9. Doan S, Gabison E, Gatinel D, et al. Topical cyclosporine A in severe steroid-dependent childhood phlyctenular keratoconjunctivitis. Am J Ophthalmol. 2006; 141:62–6.
Article10. Zaidman GW, Brown SI. Orally administered tetracycline for phlyctenular keratoconjunctivitis. Am J Ophthalmol. 1981; 92:178–82.
Article11. Koo GH, Lee JS. Treatment of phlyctenular keratoconjunctivitis with oral tetracycline in recurrent phlyctenulosis. J Korean Ophthalmol Soc. 2003; 44:2675–9.12. Thygeson P, Fritz MH. Cortisone in the treatment of phlyctenular keratoconjunctivitis. Am J Ophthalmol. 1951; 34:357–60.
Article13. Philip RN, Comstock GW, Shelton JH. Phlyctenular aberrations among Eskimos in Southwestern Alaska. I. Epidemiologic Characteristics. Am Rev Respir Dis. 1965; 91:171–87.14. Reza M, Sheridan L. Phlyctenular keratoconjunctivitis and marginal staphylococcal keratitis. Krachmer J, Mannis M, Holland E, editors. Cornea;Second ed.2005. p. 1235–8.15. Reilly CD, Mannis MJ, Steven DC. Toxic conjunctivitis. In: Krachmer J, Mannis M, Holland E, eds. Cornea. Second ed.2005. 705–7.16. Rohatgi J, Dhaliwal U. Phlyctenular eye disease: a reappraisal. Jpn J Ophthalmol. 2000; 44:146–50.
Article17. Thygeson P. The etiology and treatment of phlyctenular aberrations. Am J Ophthalmol. 1951; 34:1217–36.18. Bjorkenheim B. On precipitating factors in phlyctenular aberrations. A study on the role of tuberculosis and streptococcal and staphylococcal infection in phlyctenular disease. Acta Ophthalmol Suppl. 1951; 36:1–78.19. Culbertson WW, Huang AJ, Mandelbaum SH, et al. Effective treatment of phlyctenular keratoconjunctivitis with oral tetracycline. Ophthalmology. 1993; 100:1358–66.
Article20. Donnenfeld E, Pflugfelder SC. Topical ophthalmic cyclosporine: pharmacology and clinical uses. Surv Ophthalmol. 2009; 54:321–38.21. Cosar CB, Laibson PR, Cohen EJ, et al. Topical cyclosporine in pediatric keratoplasty. Eye Contact Lens. 2003; 29:103–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of Phlyctenular Keratoconjunctivitis with Oral Tetracycline in Recurrent Phlyctenulosis
- Clinical Aspects of Phlyctenular Keratoconjunctivitis Using a Tear Film Interferometer
- Corneal Perforation in Phlyctenular Keratitis
- Therapeutic Effect of Cyclosporine A Eyedrops in Vernal Keratoconjunctivitis
- The Therapeutic Effects of a 0.03% Tacrolimus Ointment on Childhood Phlyctenular Keratitis
