Upper Eyelid Reconstruction Using the Medpor(R) Sheet and Median Forehead Flap
- Affiliations
-
- 1Department of Ophthalmology, College of Medicine, Keimyung University, Daegu, Korea. changsd@dsmc.or.kr
- KMID: 2212502
- DOI: http://doi.org/10.3341/jkos.2009.50.7.1105
Abstract
- PURPOSE
To report the upper eyelid reconstruction with median forehead flap and Medpor(R) sheet implant following full-thickness eyelid defect resulting from tumor resection. CASE SUMMARY: A 65-year-old woman was examined at our hospital for a recurrent mass on the right upper eyelid. A wide tumor excision with a 3 mm margin and an eyelid reconstruction procedure were performed after a frozen section biopsy revealed a malignancy. The full-thickness eyelid defect was reconstructed with a median forehead flap as a substitute for skin and muscle and a Medpor(R) sheet substituted for tarsal plate was sutured with a lower conjunctiva flap for posterior lamella. The histopathology diagnosis of the lesion showed a well-differentiated squamous cell carcinoma. The lower conjunctiva was separated at 2 weeks after surgery, and then the median forehead flap detached from the upper eyelid skin at 8 weeks after surgery. One year postoperatively, there was no evidence of a wound infection and an exposure of the Medpor(R) sheet. The eyelid had a good cosmetic contour and the movement of the eyelid during blinking was natural. CONCLUSIONS: The use of a Medpor(R) sheet as a substitute for a tarsal plate in reconstructive procedures of the upper eyelid defect shows cosmetic and functional success.
MeSH Terms
Figure
-

Figure 1. Preoperative photography. (A-C) An ovoid shaped nodular mass is located in the right upper eyelid. (D) The tumor is extended into the upper eyelid margin and the palpebral conjunctiva.

Figure 2. Intraoperative photography. (A) About 18×12 mm-sized full thickness eyelid defect occurred after wide tumor resection. (B) A lower conjunctival advancement flap (white arrow) was made by starting an incision 4 mm from lid margin and dissection of a conjunctiva from lower tarsal plate. (C) The conjunctival flap was advanced and sutured at upper lid defect. (D) A Medpor® sheet was used as a substitute for the tarsal plate. (E) An anterior lamellar graft was harvested from the median forehead and sutured without tension on the pedicle flap. (F) An upper eyelid reconstruction was completed using forehead median flap, Medpor® sheet and lower conjunctival flap.

Figure 3. Photomicrographs of a section of tumor. (A) Microscopic findings of the upper eyelid show irregular clusters of anaplastic squamoid tumor cells infiltrating into the deep dermis (hematoxylin-eosin, ×100). (B) High power view of tumor mass shows keratinization of single cells (arrow) and intercellular bridge (thick arrow) in squamoid tumor cell sheets (hematoxylin-eosin, ×400).
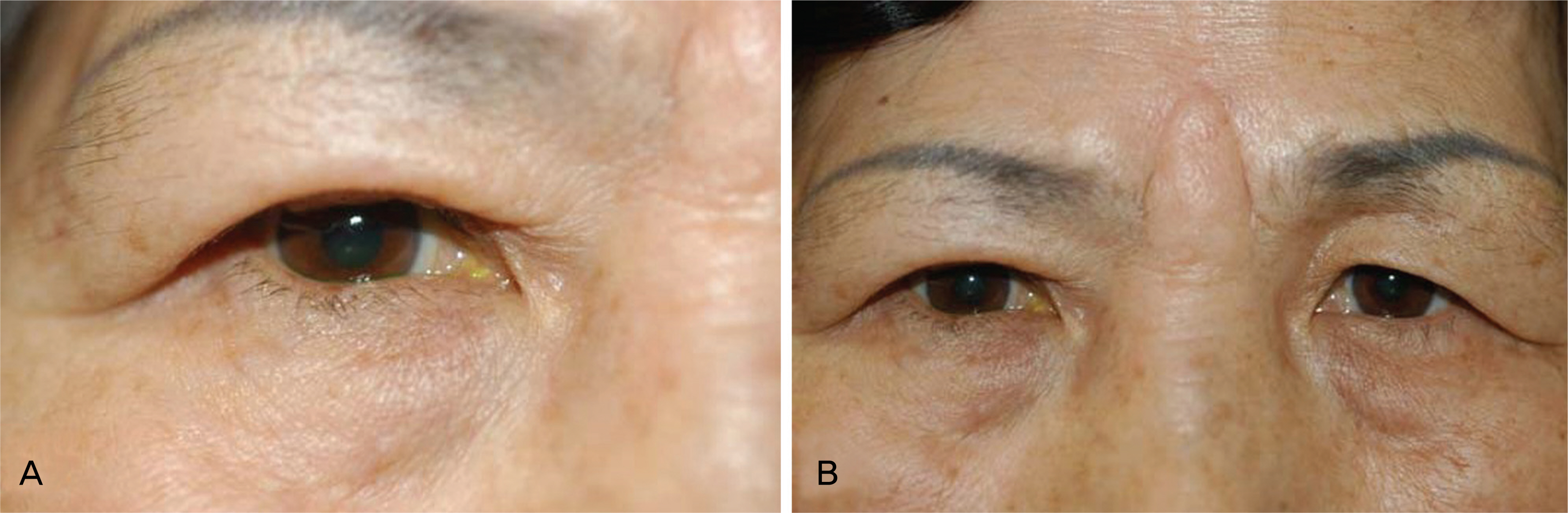
Figure 4. At 1 year postoperative photography. (A) An upper eyelid contour seems like normal feature after separation of median forehead flap. (B) There is a V-shaped mark on the glabella due to using median forehead flap in reconstructive procedure of the upper eyelid.
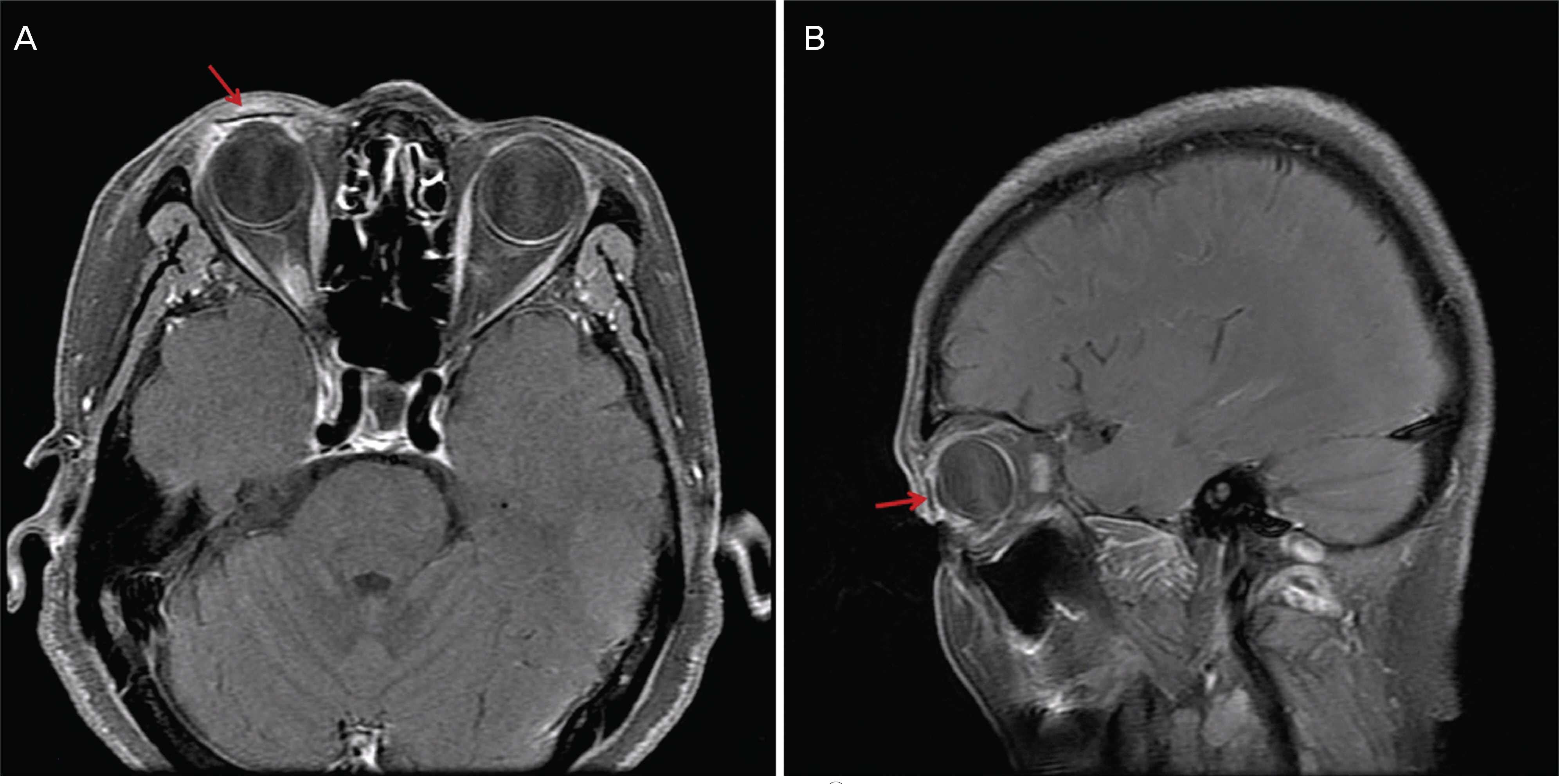
Figure 5. Postoperative magnetic resonance image. A Medpor® sheet (thick arrow) is well placed in the right upper eyelid (A, T1-weighted axial thin fat saturation image with a Gadolinium enhancement, B, T1-weighted sagittal thin fat saturation image with a Gadolinium enhancement).
Cited by 1 articles
-
The Effects of Commodified Growth Factor Products on the Fibrovascularization of Porous Polyethylene Orbital Implants
Won Mo Gu, Joon Hyuk Choi, Jun Hyuk Son
J Korean Ophthalmol Soc. 2014;55(9):1366-1371. doi: 10.3341/jkos.2014.55.9.1366.
Reference
-
References
1. McCord CD Jr, Wesley R. Reconstruction of the upper eyelid and medial canthus. McCord CD, Tanenbaum M., editorsOculoplastic Surgery. 2nd ed.New York: Raven Press;1987. chap.p. 3.2. Remano JJ, Iliff NT, Manson PN. Use of Medpor porous polyethylene implants in 140 patients with facial fracture. J Craniofac Surg. 1993; 4:142–7.3. Karesh JW, Dresner SC. High-density porous polyethylene (Medpor) as a successful anophthalmic socket implant. Ophthalmology. 1994; 101:1688–96.
Article4. Alwitry A, West S, King J, et al. Long term follow-up porous polyethylene spherical implants after enucleation and evisceration. Ophthal Plast reconstr Surg. 2007; 23:11–5.5. Odum BC, Bussard GM, Lewis RP, et al. High-density porous polyethylene for facial bone augmentation. J Long Term Eff Med Implant. 1998; 891:3–17.6. McCord CD Jr, Codner MA. Free tissue graft. McCord CD, editorEyelid surgery: principles and techniques. 3rd ed.Philadelphia: Lippincott-Raven;1995. chap.p. 3.7. Lee HB, Kwon KY, Chung SK. Reconstruction of the lower eyelid utilizing a chondromucosa after removal of squamous cell carcinoma. J Korean Ophthalmol Soc. 1985; 26:111–5.8. Park WC, Han SK, Kim NJ, et al. Effect of basic fibroblast growth factor on fibrovascular ingrowth into porous polyethylene anophthalmic socket implants. Korean J Ophthalmol. 2005; 19:1–8.
Article9. Kim HS, Ryu YA, Woo JS, et al. Comparative observation of barrier sheet and nonbarrier sheet Medpor® inserted on orbital floor in rabbits. J Korean Soc Plast Reconstr Surg. 2004; 31:682–6.10. Lim J-Y, Jang JW, Moon SH. Lid reconstruction using the porous polyethylene (Medpor®) sheet. J Korean Ophthalmol Soc. 2003; 44:2111–6.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effects of Medpor(R) Sheet as Substitute for Tarsus in Eyelid Reconstruction
- Lid Reconstruction Using the Porous Polyethylene (Medpor(R)) Sheet
- Simultaneous Upper and Lower Eyelid Reconstruction for Eyelid Defects Following a Dog Bite
- Clinical Experience of Orbital wall Reconstruction using Medpor(R) Barrier Sheet Implant
- Comparative Observation of Barrier Sheet and Nonbarrier Sheet Medpor(R) Inserted on Orbital Floor in Rabbits
