Simultaneous Upper and Lower Eyelid Reconstruction for Eyelid Defects Following a Dog Bite
- Affiliations
-
- 1Department of Ophthalmology, Yeungnam University College of Medicine, Daegu, Korea. sjh@med.yu.ac.kr
Abstract
- PURPOSE
While the principles of eyelid reconstruction are well established, the rapid choice of a method of upper and lower eyelid defect reconstruction is difficult. The authors present a successful case of simultaneous reconstruction of upper and lower eyelid defects with a modified paramedian forehead flap resulting from a dog bite.
CASE SUMMARY
The authors report a case of a 77-year-old woman with total hyphema and extensive skin defects involving the forehead, cheek, and upper and lower eyelid resulting from a dog bite. The wound on the left periorbital area was treated with microimplantation and skin grafts from the left thigh and groin. In the weeks following, sequential failure of the flap and skin graft was observed, and exposed keratitis worsened, resulting in corneal perforation. Evisceration with hydroxyapatite implantation and paramedian forehead flap was performed. After 3 weeks, division of the pedicle, transverse division of the flap, and socket reconstruction were performed.
CONCLUSIONS
Reconstruction of large, full thickness defects of both upper and lower eyelids with a paramedian forehead flap is associated with a good cosmetic outcome. Paramedian forehead flap should be considered as an effective choice for simultaneous upper and lower eyelid reconstruction.
MeSH Terms
Figure
-

Figure 1 A 77-year-old woman with total hyphema and extensive skin defect involving the forehead, cheek, upper and lower eyelid resulting from a dog bite.
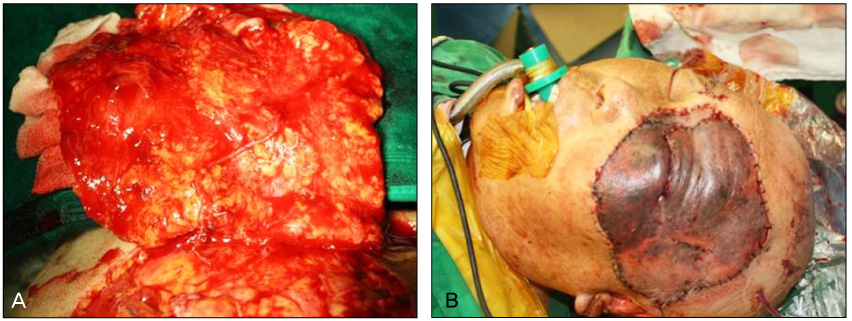
Figure 2 The stump was microimplanted on the left periorbital and temporal area.
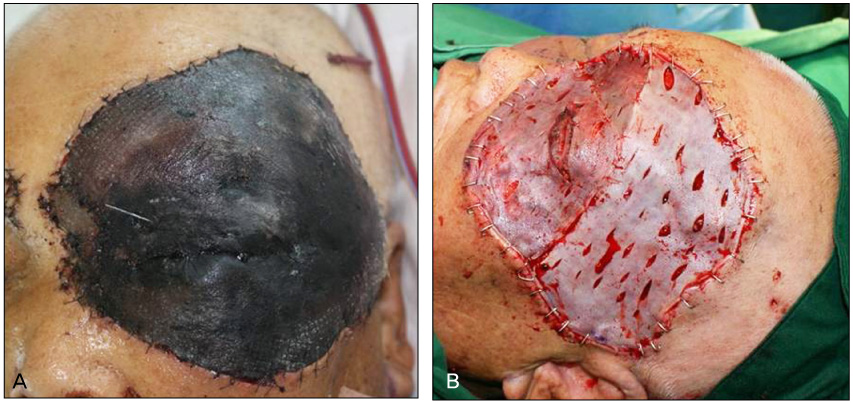
Figure 3 (A) Postoperative day 3, implanted skin necrosis is observed. (B) Debridement and skin graft from the left thigh and groin was performed (14 × 10 cm, split thickness skin graft).

Figure 4 After 7 weeks, the focal central area graft failure is found. Exposed keratitis was worsened further and resulted in corneal perforation. Modified paramedian forehead flap for eyelid reconstruction and evisceration was performed. (A) Pre-operative design. Drawing of the flap and surgical incisions. (B) The flap was harvested from the contralateral paramedian forehead. (C) Evisceration with hydroxyapatite implantation was performed. (D) Sutured without tension on the pedicle flap. (E) Postoperative photograph at 6 days.

Figure 5 The division of the pedicle. (A) Preoperative photograph. (B) Just after the operation.
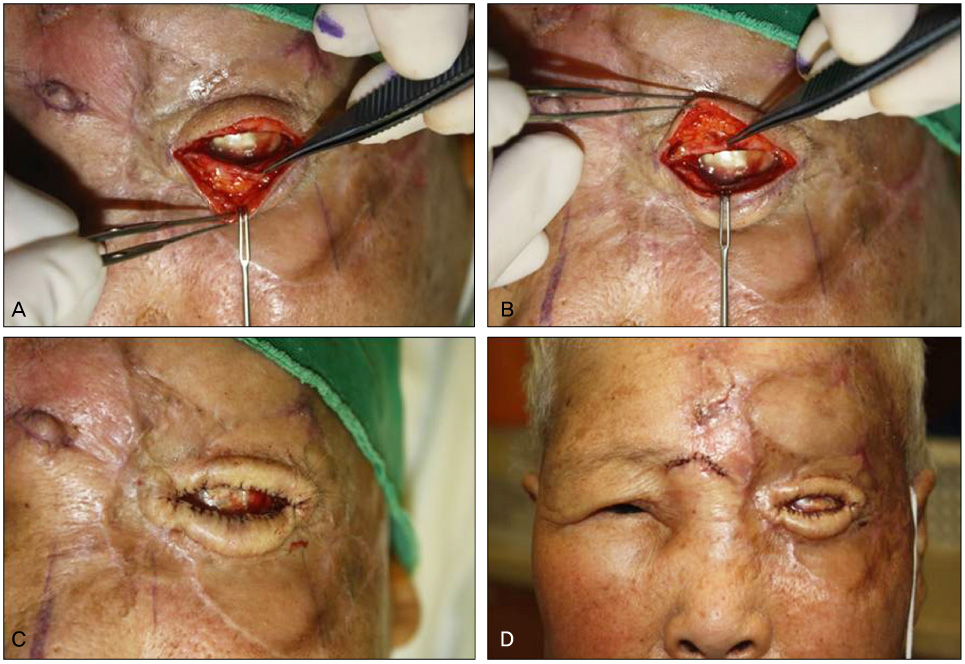
Figure 6 Eyelid and socket reconstruction. (A, B) The transverse division of the flap. (C) The flap edge was anchored to the remnant bulbar conjunctiva with sutures. (D) Postoperative photograph at 1 day.
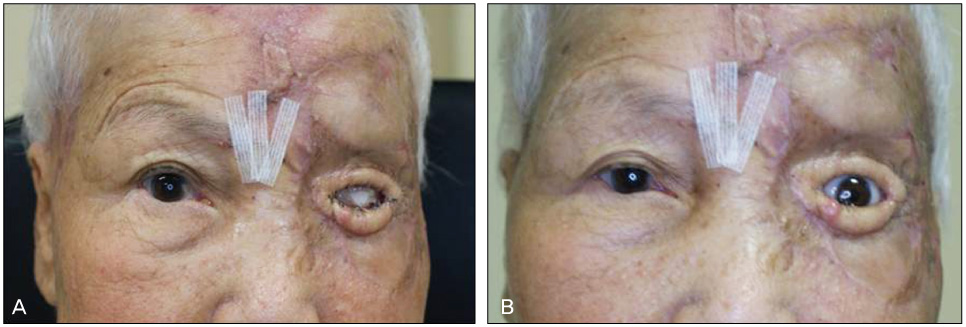
Figure 7 (A) 1 month postoperative photograph. (B) Aesthetic rehabilitation with ocular artificial prosthesis.
Reference
-
1. Kakizaki H, Madge SN, Mannor G, et al. Oculoplastic surgery for lower eyelid reconstruction after periocular cutaneous carcinoma. Int Ophthalmol Clin. 2009. 49:143–155.2. Mustardé JC. Reconstruction of eyelids. Ann Plast Surg. 1983. 11:149–169.3. Cutler NL, Beard C. A method for partial and total upper lid reconstruction. Am J Ophthalmol. 1955. 39:1–7.4. Tenzel RR, Stewart WB. Eyelid reconstruction by the semicircle flap technique. Ophthalmology. 1978. 85:1164–1169.5. Brusati R, Colletti G, Redaelli V. Upper eyelid reconstruction with forehead galeal flap. J Plast Reconstr Aesthet Surg. 2009. 62:901–905.6. Bennett SP, Richard BM, Graham KE. Median forehead flaps for eyelid reconstruction. Br J Plast Surg. 2001. 54:733–734.7. Han K. Total reconstruction of a partial-thickness upper eyelid defect with the expanded forehead flap. Ann Plast Surg. 1997. 39:24–29.8. Sakai S, Soeda S, Matsukawa A. Refinements of the island median forehead flap for reconstruction of the medial canthal area. J Dermatol Surg Oncol. 1989. 15:524–530.9. Onaran Z, Yazici I, Karakaya EI, Cavusoglu T. Simultaneous reconstruction of medial canthal area and both eyelids with a single transverse split forehead island flap. J Craniofac Surg. 2011. 22:363–365.10. Müllner K, Langmann G. Chondroplast. A new material for eyelid reconstruction. Ophthalmologica. 1999. 213:189–193.11. Yoon HJ, Kim SJ, Yoon SW, Yoon YS. Effects of Medpor(R) sheet as substitute for tarsus in eyelid reconstruction. J Korean Ophthalmol Soc. 2009. 50:1098–1104.12. Jang JH, Chang SD. Upper eyelid reconstruction using the Medpor(R) sheet and median forehead flap. J Korean Ophthalmol Soc. 2009. 50:1105–1110.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Eyelid Reconstruction by the Semicircular Flap
- Management of human bite injury of the upper and lower eyelids: a rare case report
- Composite Graft for Eyelid Reconstruction
- Reverse Modified Hughes Procedure for Reconstruction of Upper Eyelid
- Effects of Medpor(R) Sheet as Substitute for Tarsus in Eyelid Reconstruction
