A Case of Pituitary Mucormycosis in Diabetic Patient with Acromegaly and Gastric Cancer
- Affiliations
-
- 1Department of Internal Medicine, Kosin University College of Medicine, Korea.
- 2Department of Pathology, Kosin University College of Medicine, Korea.
- KMID: 2200737
- DOI: http://doi.org/10.3803/jkes.2006.21.3.245
Abstract
- Rhino-orbito-cerebral mucormycosis (ROCM) is an uncommon, acute, and aggressive fungal infection occurring in several immunocompromised states including poorly controlled diabetes. ROCM causes a very high residual morbidity and mortality due to the angioinvasion property of the fungus. Acromegaly is a chronic condition resulting from the excessive secretion of growth hormone, generally from pituitary adenoma. Although it has been demonstrated that acromegalic patients have an increased risk of neoplasm, gastric cancer with acromegaly is very rare. We experienced a case of pituitary mucormycosis in the diabetic patient with acromegaly and gastric cancer. The patient was treated successfully with subtotal gastrectomy for early gastric cancer, transsphenoidal surgery for pituitary adenoma, and a systemic application of amphotericin B for the mucormycosis.
MeSH Terms
Figure
-
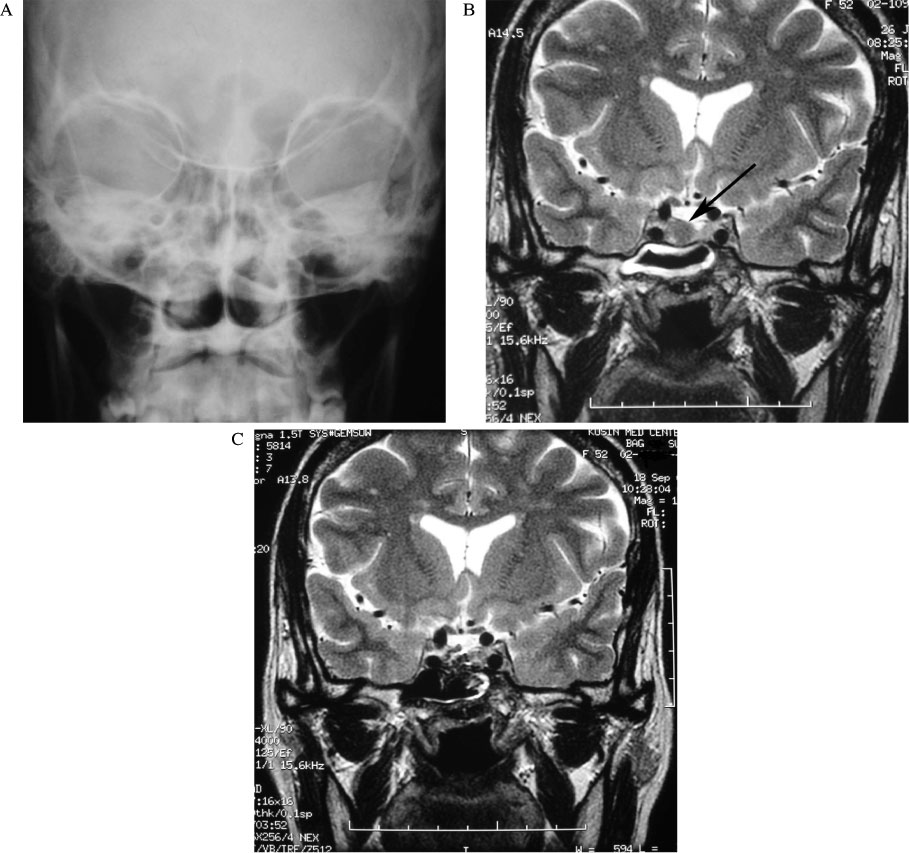
Fig. 1 A. Caldwell view shows no air fluid level in sinus. B. Sella MRI shows 0.3×0.5 cm sized mass (arrow) at the right side of pituitary gland. C. Sella MRI after transsphenoidal surgery.

Fig. 2 Endoscopic finding. An irregular and hyperemic depression with a small ulceration on center and abnormalities of the surrounding folds, such as interruption and clubbing are noted on the lesser curvature side of the proximal antrum (arrow).
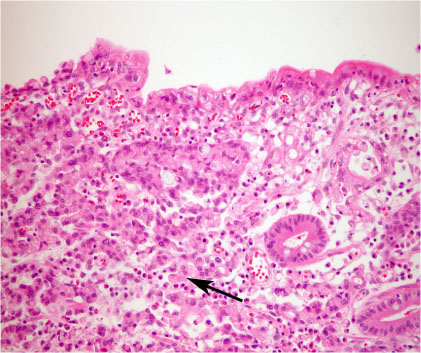
Fig. 3 Microscopic features of resected stomach. Signet ring cell type of gastric adenocarcinoma confined within the mucosa in gastrectomy specimen (H&E stain, ×200)
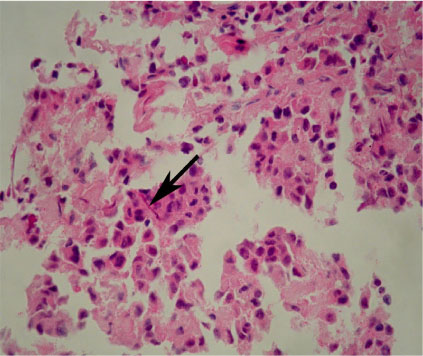
Fig. 4 A microscopic finding of the pituitary adenoma, with acidophilic cells arranged in clusters or in trabecular pattern and some hyphae (arrow) (H&E stain, ×400).
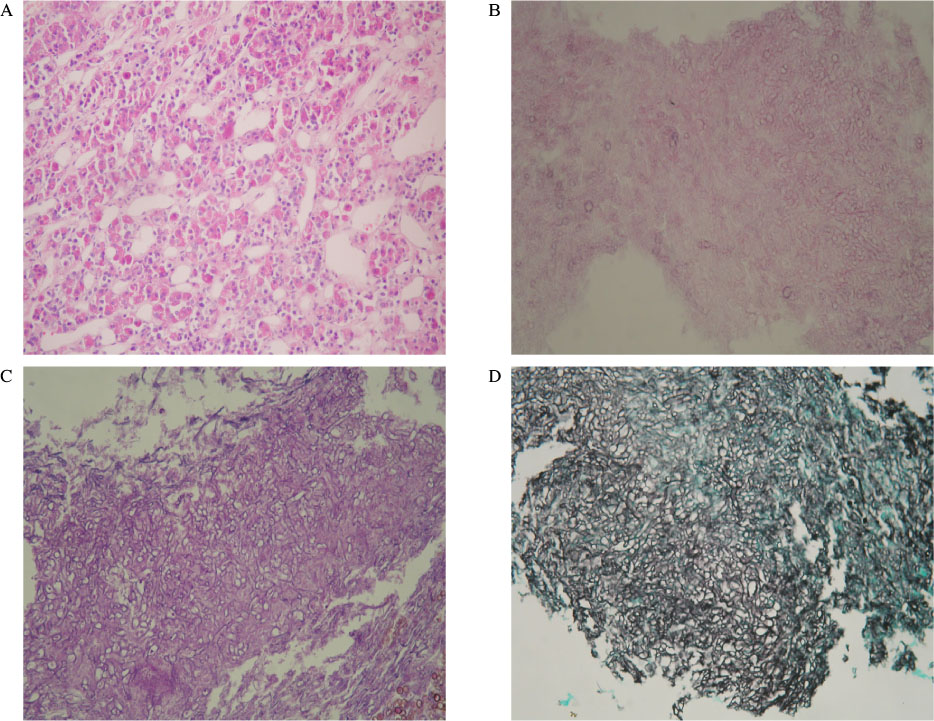
Fig. 5 Microscopic features of removed pituitary adenoma. A, pituitary gland parenchyme (H&E stain, ×200); B, mucormycosis with broad, non-septated hyphae (H&E stain, ×400); C and D, well defined hyphae contour (PAS stain, ×400 and GMS stain, ×400, respectively).
Reference
-
1. Rifkind D, Marchioro T, Schneck SA, Hill RB Jr. Systemic fungal infection complicating renal transplantation and immunosuppressive therapy. Am J Med. 1967. 43:28–38.2. Meyer RD, Rosen P, Armstrong D. Phycomycosis complication leukemia and lymphoma. Ann Intern Med. 1972. 77:871–879.3. Yohai RA, Bullock JD, Aziz AA, Markert RJ. Survival factors in rhino-orbital-cerebral mucormycosis. Surv Ophthalmol. 1994. 39:3–22.4. Ferry AP, Abedi S. Diagnosis and management of rhino-orbito-cerebral mucormycosis (phycomycosis): A report of 16 personally observed cases. Ophthalmology. 1983. 90:1096–1104.5. Ferguson BJ. Mucormycosis of the nose and paranasal sinuses. Otolaryngol Clin North Am. 2000. 33:349–365.6. Colao A, Ferone D, Marzullo P, Lombardi G. Systemic complications of acromegaly: epidemiology, pathogenesis, and management. Endocr Rev. 2004. 25:102–152.7. Baris D, Gridley G, Ron E, Weiderpass E, Mellemkjaer L, Ekbom A, Olsen JH, Baron JA, Fraumeni JF Jr. Acromegaly and cancer risk: A cohort study in Sweden and Denmark. Cancer Causes Control. 2002. 13:395–400.8. Arya KR, Pathare AV, Chadda M, Menon PS. Diabetes in acromegaly - a study of 34 cases. J Indian Med Assoc. 1997. 95:546–547.9. Ko GT, Yeung VT, Chow CC, Cockram CS. Clinical characteristics of acromegaly in Hong Kong. Endocr Res. 1999. 25:195–206.10. Ron E, Gridley G, Hrubec Z, Page W, Arora S, Fraumeni JF Jr. Acromegaly and gastrointestinal cancer. Cancer. 1991. 68:1673–1677.12. Lee JH, Park YS, Kim KM, Kim KJ, Ahn CH, Lee SY, Choi KH. Pituitary aspergillosis mimicking pituitary tumor. Am J Roentgenol. 2000. 175:1570–1572.13. Bhansali A, Bhadada S, Sharma A, Suresh V, Gupta A, Singh P, Chakarbarti A, Dash RJ. Presentation and outcome of rhino-orbital-cerebral mucormycosis in patients with diabetes. Postgrad Med J. 2004. 80:670–674. In: Gregory JL, Golden A, Haymaher W: Mucormycosis of the central nervous system: a report of three cases. Bull John Hopkins Hosp 73:302-313, 1943.14. Cohen SG, Greenberg MS. Rhinomaxillary mucormycosis in a kidney transplant patient. Oral Surg Med Pathol. 1980. 50:33–38.15. Abramson E, Wilson D, Arky RA. Rhinocerebral phycomycosis in association with diabetic ketoacidosis. Ann Intern Med. 1967. 66:735–742.16. Groote CA. Rhinocerebral phycomycosis. Arch Otolaryngol. 1970. 92:288–292.17. Blitzer A, Lawson W, Meyers BR, Biller HF. Patient survival factors in paranasal sinus mucormycosis. Laryngoscope. 1980. 90:635–648.18. Lehrer RI, Howard DH, Sypherd PS. Mucormycosis. Ann Intern Med. 1980. 93:93–108.19. Ericsson M, Anniko M, Gustafsson H, Hjalt CA, Stenling R, Tarnvik A. A case of chronic progressive rhinocerebral mucormycosis treated with liposomal amphotericin B and surgery. Clin Infect Dis. 1993. 16:585–586.20. Ramos-Gabatin A, Jordan RM. Primary pituitary aspergillosis responding to transsphenoidal surgery and combined therapy with amphotericin-B and 5-fluorocytosine. J Neurosurg. 1981. 54:839–841.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Early Gastric Cancer Coincidentally Developed in a Patient with Acromegaly
- Gastric Perforation due to Mucormycosis in a Patient with Diabetic Ketoacidosis and Chronic Pancreatitis
- A Case of Acromegaly Presenting with Diabetic Ketoacidosis
- A Case of Acromegaly Caused by Mixed Gangliocytoma-Adenoma of the Pituitary Gland
- A Case of Gastric Mucormycosis Induced Necrotic Gastric Ulcer in Patients with Diabetic Ketoacidosis
