The Change of Thyroid Hormone by Short-term Antithyroid Drug Treatment for Preoperative Euthyroidism in TSH-secreting Pituitary Adenoma
- Affiliations
-
- 1Department of Internal Medicine, Chonbuk National University Medical School, Jeonju, Korea.
- KMID: 2200566
- DOI: http://doi.org/10.3803/jkes.2005.20.3.261
Abstract
- Preoperative euthyroidism is needed to minimize the risk of intraoperative and postoperative complications, such as thyroid storm by surgery. Antithyroid drugs or steroid hormones are commonly used in primary hyperthyroidism for euthyroidism. However, there is no definite consensus for the preoperative management of a TSH secreting pituitary adenoma for the restoration of euthyroidism. Antithyroid drugs are not used for long-term the management of a TSH secreting pituitary adenoma, as they may cause rapid growth and greater invasiveness of the tumor due to a feedback mechanism, but they can be used for short-term management before neurosurgery. We experienced one case of a TSH secreting pituitary adenoma, which showed rapid free thyroid hormone increase due to the short term administration of antithyroid drugs for only 10 days. A somatostatin analogue, octreotide at a dose of 0.1mg, twice a day, was then tried. About 4 weeks later, her serum TSH and free T4 had normalized, with a concomitant clinical improvement. She subsequently underwent an uncomplicated trans-sphenoidal resection of the pituitary adenoma. Antithyroid drugs can induce a rapid thyroid hormone increase, but can only be used for a short-term period, so they should be administered with caution or their use reconsidered
MeSH Terms
Figure
-
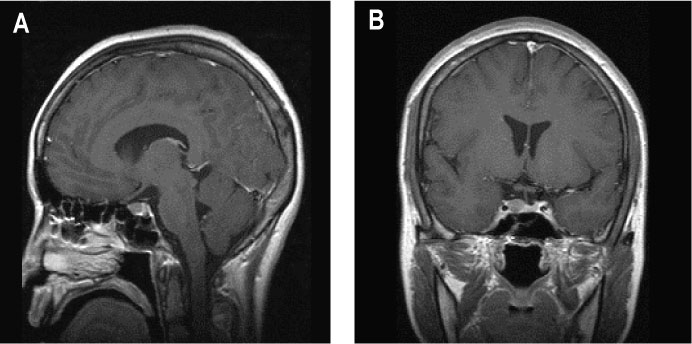
Fig. 1 Preoperative sellar MRI. (A) 12.1x8.6mm sized mass in sellar and suprasellar area in T2 weighted enhanced sagittal section image. (B) 10.6×11.5 mm sized mass in sellar and suprasellar area in T2 weighted enhanced coronal section image.
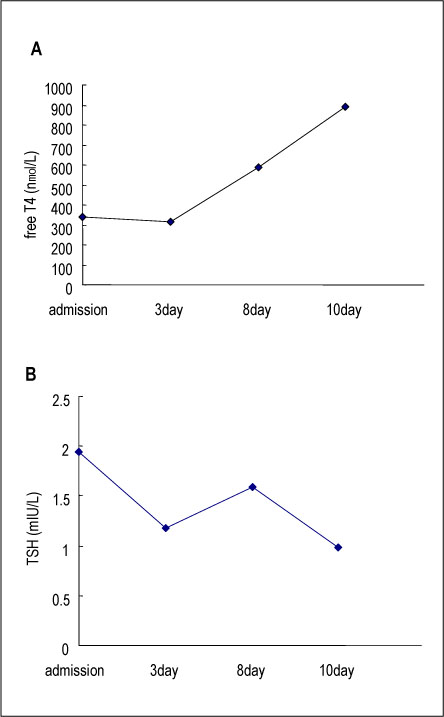
Fig. 2 (A) Free T4 levels during PTU administration (normal range 94~250 nmol/L) (B) TSH levels during PTU administration (normal range 0.17~4.05 mU/L).
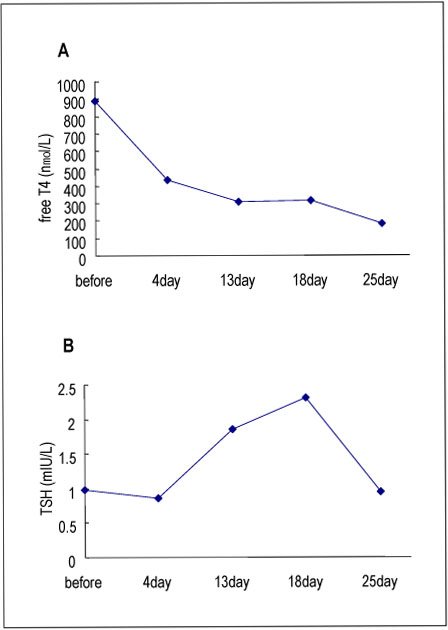
Fig. 3 (A) Free T4 levels during octreotide treatment. (B) TSH levels during octreotide treatment.
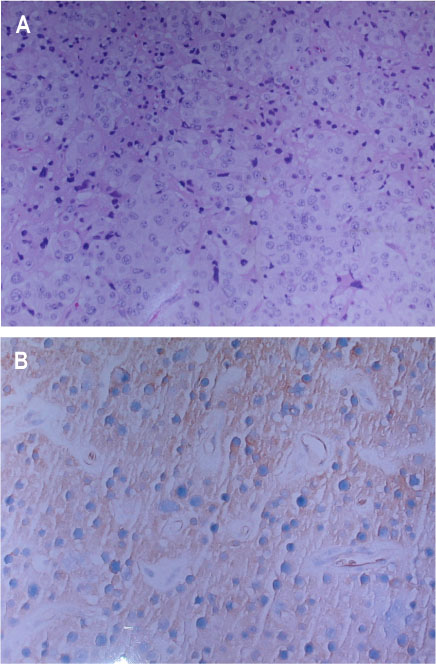
Fig. 4 Histological examination and immunohistochemical stain of tumor tissue. (A) Hematoxylin & eosin staining of tissue shows chromophobe adenoma of solid type (×100). (B) Immunohistochemical stain of tumor shows positive staining with antibodies to TSH (×200).
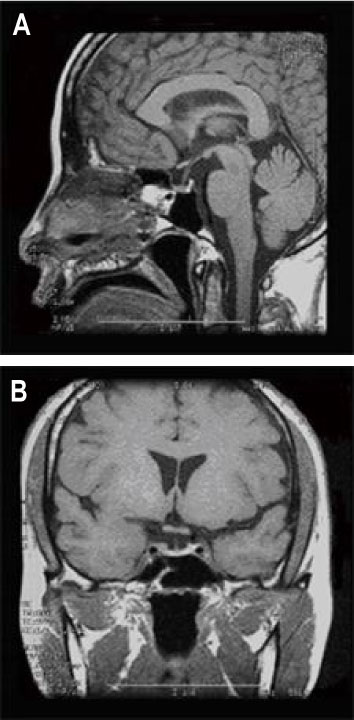
Fig. 5 Postoperative sellar MRI. (A) T1 weighted enhanced sagittal section image. (B) T1 weighted enhanced coronal section image.
Reference
-
1. Larsen PR, Kronenberg HM, Melmed S, Polonsky KS. Endocrinology. 2002. 10th ed. Philadelphia: WB Saunders Co;250–252.2. DeGroot LJ, Jameson JL. Endocrinology. 2001. 4th ed. Philadelphia: W.B. Saunders;321–327.3. Beck-Peccoz P, Brucker-Davis F, Persani L, Smallridge RC, Weintraub BD. Thyrotropin-secreting pituitary tumors. Endocr Rev. 1996. 17:610–638.4. Brucker-Davis F, Oldfield EH, Skarulis MC, Doppman JL, Weintraub BD. Thyrotropin-secreting pituitary tumors: diagnostic criteria, thyroid hormone sensitivity, and treatment outcome in 25 patients followed at the National Institutes of Health. J Clin Endocrinol Metab. 1999. 84:476–486.5. Ronald D, Allan R. Anesthesia. 2000. 5th ed. Churchill Livingston;928–929.6. Yoshida D. Thyroid storm precipitated by trauma. J Emerg Med. 1996. 14:697–701.7. Braunwald E, Fauci AS, Kasper DL, Hauser SL, Longo DL, Jameson JL. Harrison's Principles of Internal Medicine. 2005. 16th ed. McGraw Hill;2084–2096.8. Mannavola D, Persani L, Vannucchi G, Zanardelli M, Fugazzola L, Verga U, Facchetti M, Beck-Peccoz P. Different responses to chronic somatostatin analogues in patients with central hyperthyroidism. Clin Endocrinol (Oxf). 2005. 62:176–181.9. Sarlis NJ, Gourgiotis L, Koch CA, Skarulis MC, Brucker-Davis F, Doppman JL, Oldfield EH, Patronas NJ. MR imaging features of thyrotropin-secreting pituitary adenomas at initial presentation. Am J Roentgenol. 2003. 181:577–582.10. Hirvonen EA, Niskanen LK, Niskanen MM. Thyroid storm prior to induction of anaesthesia. Anaesthesia. 2004. 59:1020–1022.11. Inukai T, Fujiwara Y, Aso Y, Yamamoto A, Takemura Y. A rare case of a thyrotropin-secreting pituitary tumor which responded to methimazole. J Med. 1998. 29:185–198.12. Sunthornthepvarakul T, Prachasilchai P, Komindr A, Ngowngarmratana S, Dansirikul R. A case of thyrotropin-secreting pituitary macroadenoma. J Med Assoc Thai. 2001. 84:897–906.13. Shimon I, Melmed S. Management of pituitary tumors. Ann Intern Med. 1998. 129:472–483.14. Braverman LE, Utiger RD. The thyroid. 2005. 9th ed. Philadelphia: Lippincott Williams & Wilkins;500–507.15. Gittoes NJ, McCabe CJ, Verhaeg J, Sheppard MC, Franklyn JA. An abnormality of thyroid hormone receptor expression may explain abnormal thyrotropin production in thyrotropin-secreting pituitary tumors. Thyroid. 1998. 8:9–14.16. Tannahill LA, Visser TJ, McCabe CJ, Kachilele S, Boelaert K, Sheppard MC, Franklyn JA, Gittoes NJ. Dysregulation of iodothyronine deiodinase enzyme expression and function in human pituitary tumours. Clin Endocrinol (Oxf). 2002. 56:735–743.17. Beckers A, Abs R, Mahler C, Vandalem JL, Pirens G, Hennen G, Stevenaert A. Thyrotropin-secreting pituitary adenomas: report of seven cases. J Clin Endocrinol Metab. 1991. 72:477–483.18. Socin HV, Chanson P, Delemer B, Tabarin A, Rohmer V, Mockel J, Stevenaert A, Beckers A. The changing spectrum of TSH-secreting pituitary adenomas: diagnosis and management in 43 patients. Eur J Endocrinol. 2003. 148:433–442.19. Kuhn J, Arlot S, Lefebvre H, Caron P, Cortet-Rudelli C, Archambaud F, Chanson P, Tabarin A, Goth M, Blumberg J, Catus F, Ispas S, Beck-Peccoz P. Evaluation of the treatment of thyrotropin-secreting pituitary adenomas with a slow release formulation of the Somatostatin analog lanreotide. J Clin Endocrinol Metab. 2000. 85:1487–1491.20. Kimvir S, Pejman C, Daniel F, Christine H, Kris V, Inder J. Treatment of Hyperthyroidism Associated with Thyrotropin-secreting Pituitary Adenomas with Iopanoic Acid. J Clin Endocrinol Metab. 2004. 89:708–711.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Characteristics and Treatments of Patients with TSH Secreting Pituitary Adenoma
- MRI of the TSH(Thyroid Stimulating Hormone) -Secreting Pituitary Adenoma
- A Case of Thyrotropin (TSH)-Secreting Pituitary Adenoma in a Patient with Ankylosing Spondylitis
- A case of pituitary resistance to thyroid hormone with nonfunctioning pituitary microadenoma
- A case of Thyrotrophin(TSH)-Secreting Giant Pituitary Adenoma: Biochemical Remission with Surgery
