Unilateral intraoral vertical ramus osteotomy and sagittal split ramus osteotomy for the treatment of asymmetric mandibles
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, Asan Medical Center, Seoul, Korea. amcomsjjh@gmail.com
- KMID: 2189474
- DOI: http://doi.org/10.5125/jkaoms.2015.41.2.102
Abstract
- In surgery for facial asymmetry, mandibles can be classified into two types, rotational and translational, according to the required mandibular movements for surgery. During surgery for rotational mandibular asymmetry, a bilateral sagittal split ramus osteotomy (BSSRO) may cause a large bone gap between the proximal and distal segments as well as condylar displacement, resulting in a relapse of the temporomandibular joint disorder, especially in severe cases. The intraoral vertical ramus osteotomy has an advantage, in this respect, because it causes less rotational displacement of the proximal segment on the deviated side and even displaced or rotated condylar segments may return to their original physiologic position. Unilateral intraoral vertical ramus osteotomy (UIVRO) on the short side combined with contralateral SSRO was devised as an alternative technique to resolve the spatial problems caused by conventional SSRO in cases of severe rotational asymmetry. A series of three cases were treated with the previously suggested protocol and the follow-up period was analyzed. In serial cases, UIVRO combined with contralateral SSRO may avoid mediolateral flaring of the bone segments and condylar dislocation, and result in improved condition of the temporomandibular joint. UIVRO combined with contralateral SSRO is expected to be a useful technique for the treatment of rotational mandibular asymmetry.
MeSH Terms
Figure
-
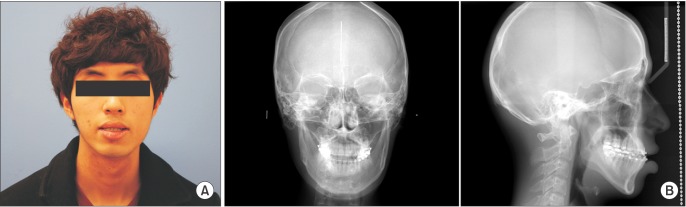
Fig. 1 Preoperative facial photograph (A) and cephalometric radiographs (B) (case 1). The patient was explained for the use of clinical images on this article and informed consent was gained.
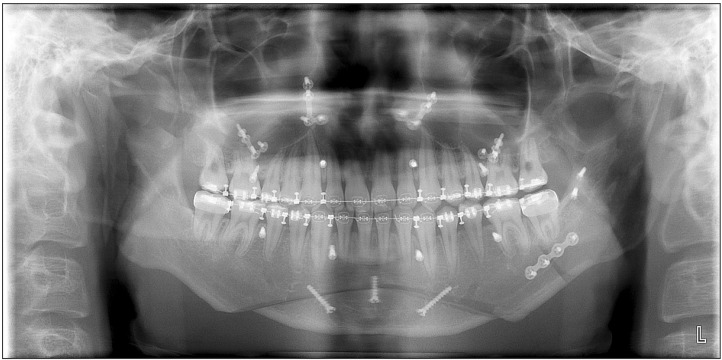
Fig. 2 Postoperative panoramic radiograph 6 weeks after surgery; intraoral vertical ramus osteotomy and coronoidotomy on the right mandible and sagittal split ramus osteotomy on the left with a miniplate and positional screw fixation.
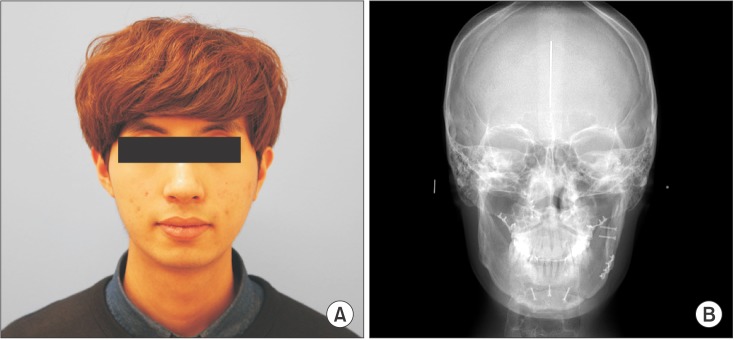
Fig. 3 Facial photograph (A) and cephalometric posterior-anterior radiograph (B) 6 months after surgery. The patient was explained for the use of clinical images on this article and informed consent was gained.
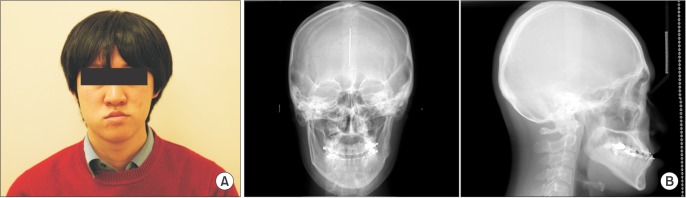
Fig. 4 Preoperative facial photograph (A) and cephalometric radiographs (B) (case 2). The patient was explained for the use of clinical images on this article and informed consent was gained.
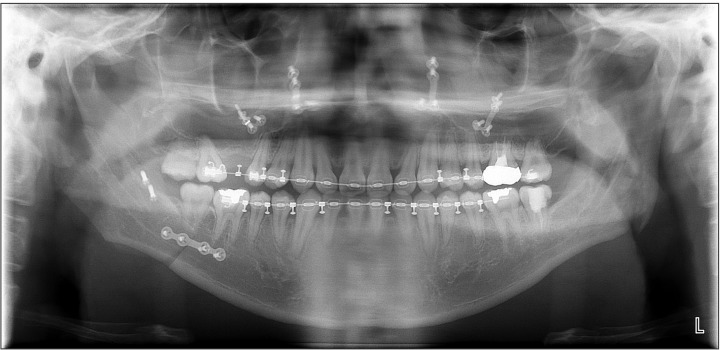
Fig. 5 Postoperative panoramic radiograph 6 weeks after surgery; intraoral vertical ramus osteotomy and coronoidotomy on the left mandible and sagittal split ramus osteotomy on the right with miniplate and positional screw fixation.
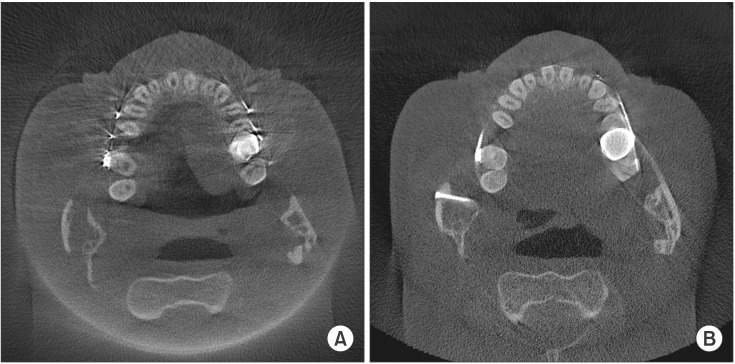
Fig. 6 Postoperative cone-beam computed tomography images. A. Postoperative 6 week; the most posterior aspect of the distal segment on the left intraoral vertical ramus osteotomy side was positioned lateral to the proximal segment rather than medially. B. Postoperative 1 year; bony union between the segments on the left as well as the right side can be seen.
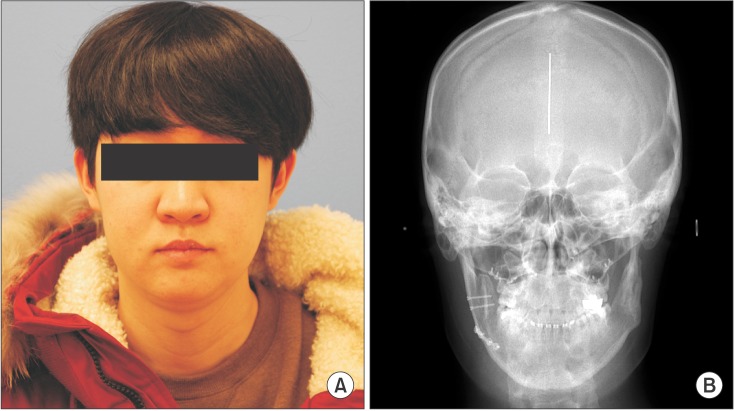
Fig. 7 Facial photograph (A) and cephalometric posterior-anterior radiograph (B) 18 months after surgery. The patient was explained for the use of clinical images on this article and informed consent was gained.
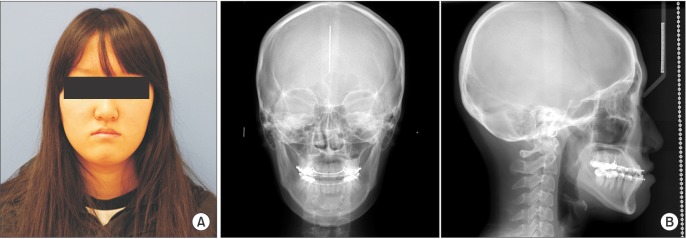
Fig. 8 Preoperative facial photograph (A) and cephalometric radiographs (B) (case 3). The patient was explained for the use of clinical images on this article and informed consent was gained.
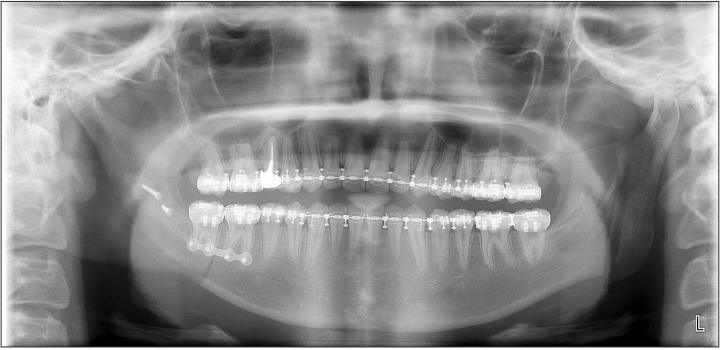
Fig. 9 Postoperative panoramic radiograph 6 weeks after surgery; intraoral vertical ramus osteotomy and coronoidotomy on the left mandible and sagittal split ramus osteotomy on the right with miniplate and positional screw fixation.

Fig. 10 Facial photograph (A) and cephalometric posterior-anterior radiograph (B) 6 months after surgery. The patient was explained for the use of clinical images on this article and informed consent was gained.
Cited by 2 articles
-
Sagittal split ramus osteotomy, intraoral vertical ramus osteotomy, and lateral corticectomy for asymmetric mandibular prognathism
Joo Young Lee, Se Jin Han
J Korean Assoc Oral Maxillofac Surg. 2021;47(4):249-256. doi: 10.5125/jkaoms.2021.47.4.249.Positional changes of the mandibular condyle in unilateral sagittal split ramus osteotomy combined with intraoral vertical ramus osteotomy for asymmetric class III malocclusion
Jun Park, Ki-Eun Hong, Ji-Eon Yun, Eun-Sup Shin, Chul-Hoon Kim, Bok-Joo Kim, Jung-Han Kim
J Korean Assoc Oral Maxillofac Surg. 2021;47(5):373-381. doi: 10.5125/jkaoms.2021.47.5.373.
Reference
-
1. Schwartz HC. Efficient surgical management of mandibular asymmetry. J Oral Maxillofac Surg. 2011; 69:645–654. PMID: 20934795.
Article2. Epker BN, Stella JP, Fish LC. Dentofacial deformities, integrated orthodontic and surgical correction. 2nd ed. St. Louis: Mosby;1999.3. Ellis E 3rd. A method to passively align the sagittal ramus osteotomy segments. J Oral Maxillofac Surg. 2007; 65:2125–2130. PMID: 17884553.
Article4. Yoshida K, Rivera RS, Kaneko M, Kurita K. Minimizing displacement of the proximal segment after bilateral sagittal split ramus osteotomy in asymmetric cases. J Oral Maxillofac Surg. 2001; 59:15–18. PMID: 11152184.
Article5. Jeon JH. Surgical treatment planning for the two subtypes of mandibular asymmetry. J Korean Assoc Oral Maxillofac Surg. 2014; 40:205. PMID: 25368831.
Article6. Ellis E 3rd, Hinton RJ. Histologic examination of the temporomandibular joint after mandibular advancement with and without rigid fixation: an experimental investigation in adult Macaca mulatta. J Oral Maxillofac Surg. 1991; 49:1316–1327. PMID: 1955923.
Article7. Ueki K, Degerliyurt K, Hashiba Y, Marukawa K, Nakagawa K, Yamamoto E. Horizontal changes in the condylar head after sagittal split ramus osteotomy with bent plate fixation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008; 106:656–661. PMID: 18602292.
Article8. Ellis E 3rd. Condylar positioning devices for orthognathic surgery: are they necessary? J Oral Maxillofac Surg. 1994; 52:536–552. PMID: 8189289.
Article9. Costa F, Robiony M, Toro C, Sembronio S, Polini F, Politi M. Condylar positioning devices for orthognathic surgery: a literature review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008; 106:179–190. PMID: 18417381.
Article10. Bell WH, Yamaguchi Y, Poor MR. Treatment of temporomandibular joint dysfunction by intraoral vertical ramus osteotomy. Int J Adult Orthodon Orthognath Surg. 1990; 5:9–27. PMID: 2373914.11. Bell WH, Yamaguchi Y. Condyle position and mobility before and after intraoral vertical ramus osteotomies and neuromuscular rehabilitation. Int J Adult Orthodon Orthognath Surg. 1991; 6:97–104. PMID: 1811034.12. Choi YS, Jung HD, Kim SY, Park HS, Jung YS. Remodelling pattern of the ramus on submentovertex cephalographs after intraoral vertical ramus osteotomy. Br J Oral Maxillofac Surg. 2013; 51:e259–e262. PMID: 24070895.
Article13. Jung HD, Jung YS, Park HS. The chronologic prevalence of temporomandibular joint disorders associated with bilateral intraoral vertical ramus osteotomy. J Oral Maxillofac Surg. 2009; 67:797–803. PMID: 19304037.
Article14. Hall HD, Navarro EZ, Gibbs SJ. Prospective study of modified condylotomy for treatment of nonreducing disk displacement. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000; 89:147–158. PMID: 10673649.
Article15. Hall HD, Navarro EZ, Gibbs SJ. One- and three-year prospective outcome study of modified condylotomy for treatment of reducing disc displacement. J Oral Maxillofac Surg. 2000; 58:7–17. PMID: 10632159.
Article16. Ueki K, Marukawa K, Shimada M, Yoshida K, Hashiba Y, Shimizu C, et al. Condylar and disc positions after intraoral vertical ramus osteotomy with and without a Le Fort I osteotomy. Int J Oral Maxillofac Surg. 2007; 36:207–213. PMID: 17239565.
Article17. Lai W, Yamada K, Hanada K, Ali IM, Takagi R, Kobayashi T, et al. Postoperative mandibular stability after orthognathic surgery in patients with mandibular protrusion and mandibular deviation. Int J Adult Orthodon Orthognath Surg. 2002; 17:13–22. PMID: 11934051.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case report of hemifacial microsomia
- Surgical correction of maxillofacial deformity with fibrous-osseous lesion of mandible using the intraoral vertical ramus osteotomy
- Treatment of osteomyelitis in the rear area of the lingula of the mandible using sagittal split ramus osteotomy: a case report
- Unilateral bimaxillary vertical elongation by maxillary distraction osteogenesis and mandibular sagittal split ramus osteotomy: a case report
- Sagittal split ramus osteotomy, intraoral vertical ramus osteotomy, and lateral corticectomy for asymmetric mandibular prognathism
