Unilateral bimaxillary vertical elongation by maxillary distraction osteogenesis and mandibular sagittal split ramus osteotomy: a case report
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, School of Dentistry, Seoul National University Dental Hospital, Dental Research Institute, BK21 for Craniomaxillofacial Life Science, Seoul National University, Seoul, Korea. sjhwang@snu.ac.kr
- KMID: 2136995
- DOI: http://doi.org/10.5125/jkaoms.2011.37.6.539
Abstract
- Maxillary canting and vertical shortening of the unilateral mandibular ramus height is common in cases of severe facial asymmetry. Normally, mandibular distraction osteogenesis (DO) with horizontal osteotomy at the ascending ramus is used for vertical lengthening of the mandibular ramus to correct facial asymmetry with an absolute shortened ascending ramus. In this case report, vertical lengthening of the ascending ramus was performed successfully with unilateral DO and sagittal split ramus osteotomy (SSRO), where the posterior part of the distal segment can be distracted simultaneously in an inferior direction with maxillary DO, resulting in a lengthening of the medial pterygoid muscle. This case describes the acquired unilateral mandibular hypoplasia caused by a condylar fracture at an early age, which resulted in abnormal mandibular development that ultimately caused severe facial trismus. The treatment of this case included two-stage surgery consisting of bimaxillary distraction osteogenesis for gradual lengthening of the unilateral facial height followed by secondary orthognathic surgery to correct the transverse asymmetry. At the one year follow-up after SSRO, the vertical length was maintained without complications.
MeSH Terms
Figure
-

Fig. 1. A, D, G. Pre-operative clinical photograph. B, E, H. At Clinical photo taken immediately after the removal of the distraction device, taken at approximately a year and 3 months after the first surgery (left condylectomy, maxillary distraction osteogenesis with Le Fort I osteotomy, and left unilateral sagittal split ramal osteotomy). C, F, I. Clinical photo taken after the second surgery (maxillary Le Fort I osteotomy, bilateral sagittal split ramal osteotomy, and autogenic bone graft using illiac bone) taken 1 year and 7 months after the first surgery, and 2½ months after the second surgery. Young-Eun Jung et al: Unilateral bimaxillary vertical elongation by maxillary distraction osteogenesis and mandibular sagittal split ramus osteotomy: a case report. J Korean Assoc Oral Maxillofac Surg 2011
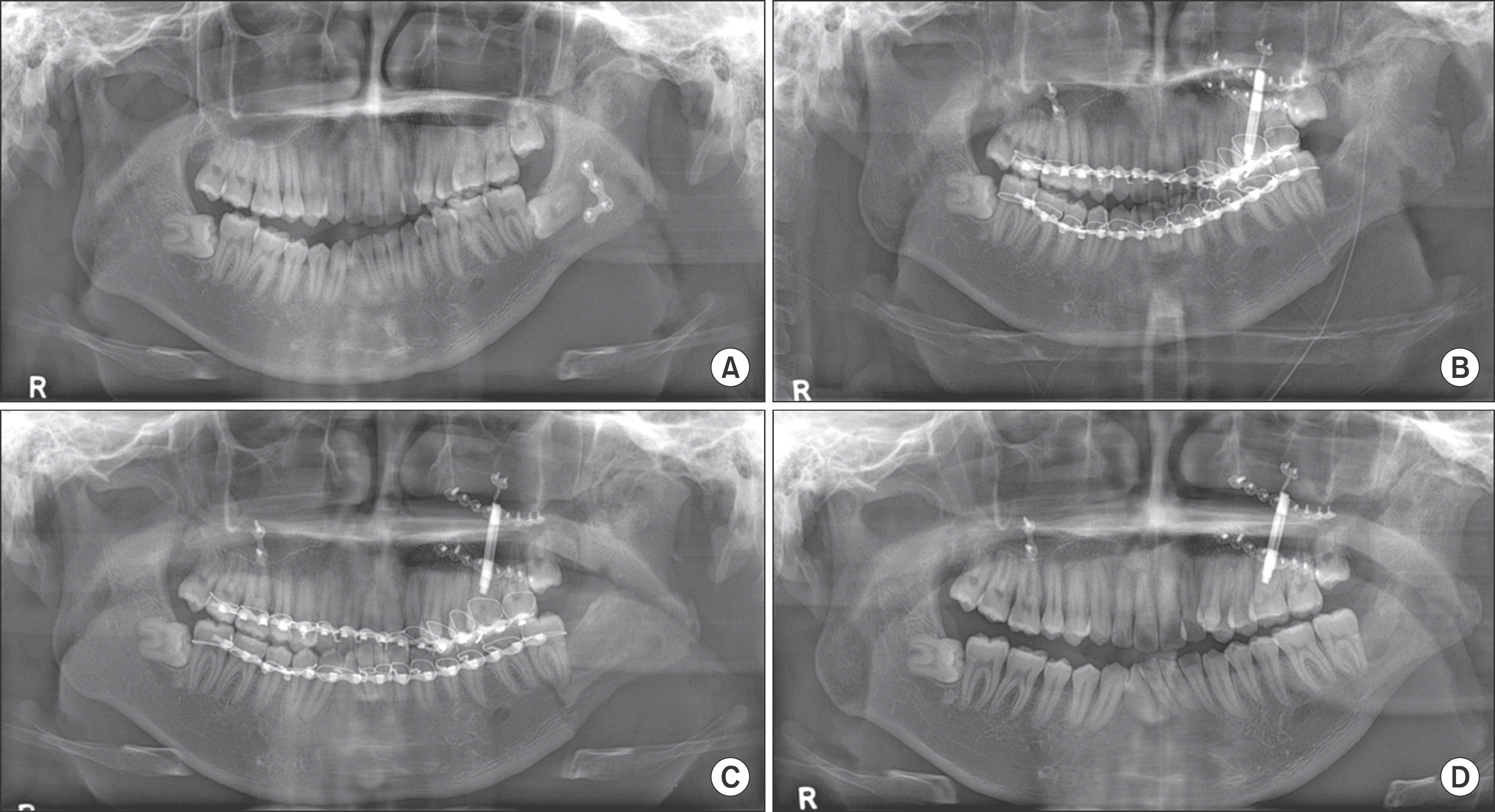
Fig. 2. A. Pre-operative radiograph. B. Radiograph taken immediately after the first surgery. Distraction device was inserted to the maxilla following Le Fort I osteotomy. Left unilateral sagittal split ramal osteotomy was done. Intermaxillary fixation was done, and distraction was initiated. C. Radiograph taken 24 days after the first surgery. The amount of maxillary distraction was 9.5 mm. D. 2½ months after the first surgery. Young-Eun Jung et al: Unilateral bimaxillary vertical elongation by maxillary distraction osteogenesis and mandibular sagittal split ramus osteotomy: a case report. J Korean Assoc Oral Maxillofac Surg 2011
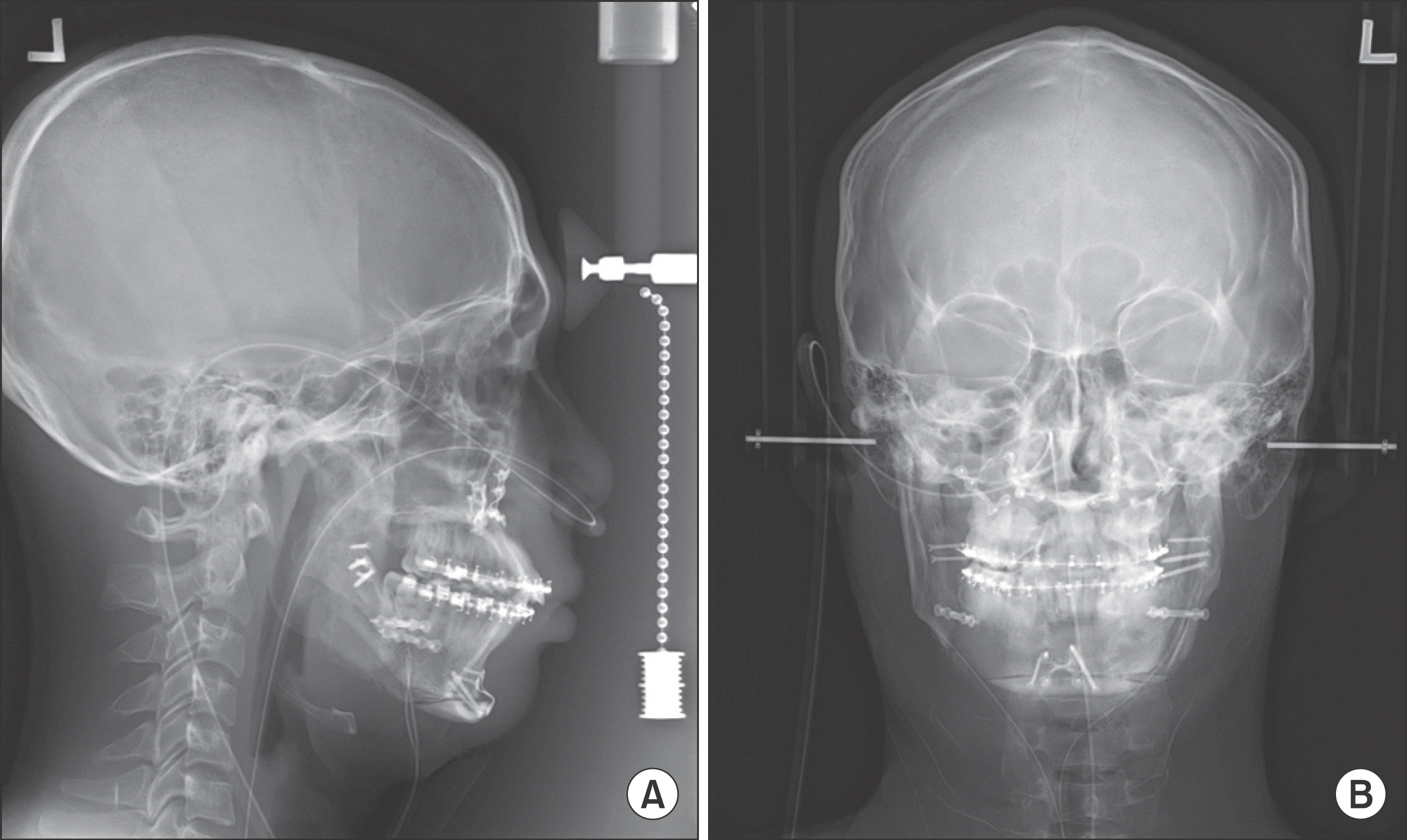
Fig. 3. Radiograph taken immediately after the second surgery (maxillary Le Fort I osteotomy, bilateral sagittal split ramal osteotomy, and autogenic bone graft using illiac bone). Young-Eun Jung et al: Unilateral bimaxillary vertical elongation by maxillary distraction osteogenesis and mandibular sagittal split ramus osteotomy: a case report. J Korean Assoc Oral Maxillofac Surg 2011
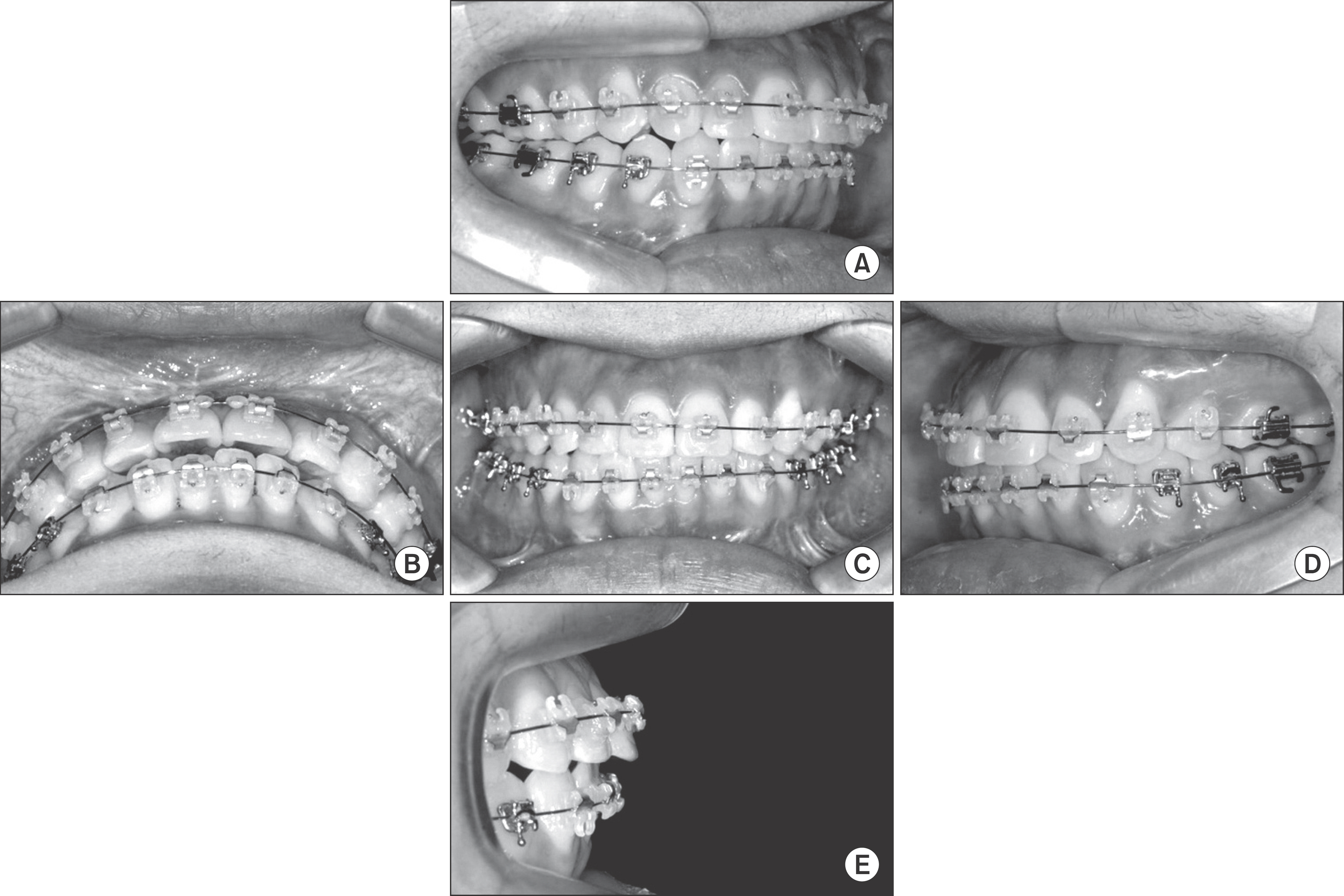
Fig. 4. Clinical photograph taken 3 months after the second surgery. Young-Eun Jung et al: Unilateral bimaxillary vertical elongation by maxillary distraction osteogenesis and mandibular sagittal split ramus osteotomy: a case report. J Korean Assoc Oral Maxillofac Surg 2011
Reference
-
References
1. Tank W, Wright D, Iizuka T. Unilateral dysplasia of the mandibular condyle: report of a case. J Oral Maxillofac Surg. 1998; 56:765–9.
Article2. Ilizarov GA. The principles of the Ilizarov method. Bull Hosp Jt Dis Orthop Inst. 1988; 48:1–11.3. McCarthy JG, Schreiber J, Karp N, Thorne CH, Grayson BH. Lengthening the human mandible by gradual distraction. Plast Reconstr Surg. 1992; 89:1–8.
Article4. Niederhagen B, Braumann B, Bergé S, von Lindern JJ, Appel T. Tooth-borne distraction to widen the mandible. Technical note. Int J Oral Maxillofac Surg. 2000; 29:27–8.
Article5. Sadakah AA, Elgazzar RF, Abdelhady AI. Intraoral distraction osteogenesis for the correction of facial deformities following temporomandibular joint ankylosis: a modified technique. Int J Oral Maxillofac Surg. 2006; 35:399–406.
Article6. Yu H, Shen G, Zhang S, Wang X. Gap arthroplasty combined with distraction osteogenesis in the treatment of unilateral ankylosis of the temporomandibular joint and micrognathia. Br J Oral Maxillofac Surg. 2009; 47:200–4.
Article7. Rao K, Kumar S, Kumar V, Singh AK, Bhatnagar SK. The role of simultaneous gap arthroplasty and distraction osteogenesis in the management of temporomandibular joint ankylosis with mandibular deformity in children. J Craniomaxillofac Surg. 2004; 32:38–42.
Article8. Papageorge MB, Apostolidis C. Simultaneous mandibular distraction and arthroplasty in a patient with temporomandibular joint ankylosis and mandibular hypoplasia. J Oral Maxillofac Surg. 1999; 57:328–33.
Article9. Yoon HJ, Kim HG. Intraoral mandibular distraction osteogenesis in facial asymmetry patients with unilateral temporomandibular joint bony ankylosis. Int J Oral Maxillofac Surg. 2002; 31:544–8.
Article10. Ortiz Monasterio F, Molina F, Andrade L, Rodriguez C, Sainz Arregui J. Simultaneous mandibular and maxillary distraction in hemifacial microsomia in adults: avoiding occlusal disasters. Plast Reconstr Surg. 1997; 100:852–61.11. Master DL, Hanson PR, Gosain AK. Complications of mandibular distraction osteogenesis. J Craniofac Surg. 2010; 21:1565–70.
Article12. Vu HL, Panchal J, Levine N. Combined simultaneous distraction osteogenesis of the maxilla and mandible using a single distraction device in hemifacial microsomia. J Craniofac Surg. 2001; 12:253–8.
Article13. Schwartz HC, Relle RJ. Distraction osteogenesis for temporomandibular joint reconstruction. Oral Maxillofac Surg. 2008; 66:718–23.
Article14. Dean A, Alamillos F. Mandibular distraction in temporomandibular joint ankylosis. Plast Reconstr Surg. 1999; 104:2021–31.
Article15. Kaban LB, Moses MH, Mulliken JB. Surgical correction of hemifacial microsomia in the growing child. Plast Reconstr Surg. 1988; 82:9–19.
Article16. Cho BC, Shin DP, Park JW, Baik BS. Bimaxillary osteodistraction for the treatment of facial asymmetry in adults. Br J Plast Surg. 2001; 54:491–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Distraction Osteogenesis of Mandible using Short-Sagittal Osteotomy for the Patient with Hemifacial Microsomia
- Comparison of Postoperative Stability between Distraction Osteogenesis and Bilateral Sagittal Split Ramus Osteotomy in Mandibular Retrognathism
- Correction of Facial Asymmetry Using Costochondral Graft and Orthognathic Surgery in Hemifacial Microsomia Patient: Case Report
- Skeletal relapse pattern after sagittal split ramus osteotomy of mandibular prognathic patient
- Unilateral intraoral vertical ramus osteotomy and sagittal split ramus osteotomy for the treatment of asymmetric mandibles
