J Korean Med Assoc.
2003 Jan;46(1):56-66. 10.5124/jkma.2003.46.1.56.
Pancreatitis
- Affiliations
-
- 1Department of Internal Medicine, Anam Hospital, Korea University College of Medicine, Korea. kumcge@cholian.net
- KMID: 2183066
- DOI: http://doi.org/10.5124/jkma.2003.46.1.56
Abstract
- Pancreatic inflammatory disease may be classified as acute pancreatitis(AP) and chronic pancreatitis(CP) by primarily clinical criteria, with the obvious difference between them being restoration of normal function in the former and permanent residual damage in the latter. Gallstones and alcohol are the most common causes of acute pancreatitis. Abdominal pain is the major symptom. The diagnosis of AP is usually established by the presence of an increased serum amylase and lipase. CT scanning is the imaging method of choice in determining the severity and complications of AP. There are no generally recognized specific treatments for AP. Supportive therapy, which includes vigorous intravenous hydration, ample analgesia, and vascular, respiratory, and renal support as needed, remains the mainstay of therapy. CP may present as episodes of acute inflammation superimposed on a previously injured pancreas or as chronic fibrotic damage with persistent pain or malabsorption. Alcoholism is the most common cause of CP. The classic triad of pancreatic calcification, steatorrhea, and diabetes mellitus usually establishes the diagnosis of CP. ERCP and pancreatic function test are gold standard imaging procedures for diagnosing CP and planning treatment. Therapy for patients with CP is directed toward major problems such as pain, malabsorption, and diabetes mellitus. Pancreatic enzyme replacement therapy improves the abdominal pain and malabsorption. If Complications is found, endoscopic or Surgical treatments should be considered.
Keyword
MeSH Terms
Figure
-
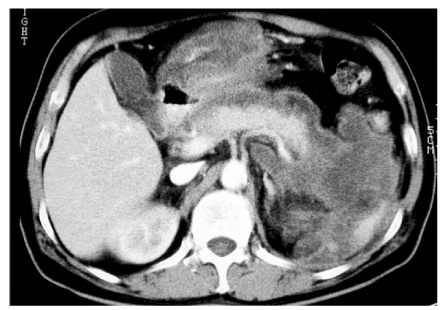
Figure 1

Figure 2

Figure 3

Figure 4
Reference
-
1. Steinberg W, Tenner S. Acute pancreatitis. N Engl J Med. 1994. 330:1198–1210.
Article3. Horiuchi A, Kawa S, Akamatsu T, Aoki Y, Mukawa K, Kiyosawa K, et al. Characteristic pancreatic duct appearance in autoimmune chronic pancreatitis: A case report and review of the Japanese literature. Am J Gastroenterol. 1998. 93:260–263.
Article4. Whitcomd DC. The first international symposium on hereditary pancreatitis. Pancreas. 1998. 18:1–12.8. Banks PA. Practice guidelines in acute pancreatitis. Am J Gastroenterol. 1997. 92:377–386.
Article9. Niederau C, Grendell JH. Diagnosis of chronic pancreatitis. Gastroenterology. 1985. 88:1973–1995.
Article11. Steer ML, Waxman I, Freedman S. Chronic pancreatitis. N Engl J Med. 1995. 332:1482–1490.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute Pancreatitis with Hypercalcemia as Initial Manifestation of Multiple Myeloma
- Acute Pancreatitis associated with Acute Hepatitis A in an Old Aged Patient
- Surgical Approach for Acute Pancreatitis
- Genetics of Pancreatitis: Are There Differences between Korea and Other Countries?
- Etiology, Pathogenesis and Natural Course of Chronic Pancreatitis
