Ewha Med J.
2015 Oct;38(3):129-132. 10.12771/emj.2015.38.3.129.
Incidentally Discovered Aldosterone and Cortisol Cosecreting Adrenal Cortical Adenoma
- Affiliations
-
- 1Department of Internal Medicine, Ewha Womans University School of Medicine, Seoul, Korea. yasung@ewha.ac.kr
- 2Department of Surgery, Ewha Womans University School of Medicine, Seoul, Korea.
- 3Department of Pathology, Ewha Womans University School of Medicine, Seoul, Korea.
- KMID: 2171351
- DOI: http://doi.org/10.12771/emj.2015.38.3.129
Abstract
- A substantial proportion of adrenal incidentalomas demonstrates subtle hormonal hypersecretion; however, adenomas that cosecrete aldosterone and cortisol are rare. We here report a case of an adrenal mass that was incidentally detected on a computed tomography scan in a 57-year-old man. The patient had a 10-year history of diabetes mellitus and a 5-year history of hypertension. Evaluation revealed hyperaldosteronemia with an elevated plasma aldosterone-to-renin ratio, hypokalemia, unsuppressed cortisol after dexamethasone administration, and elevated urinary free cortisol concentration. The appearance of the right adrenalectomy specimen indicated adrenal adenoma. Postoperatively, the blood glucose and blood pressure control improved and the urinary cortisol and aldosterone-to-renin ratio normalized. A complete endocrine evaluation in patients with incidentally discovered adrenal masses should be performed, even if the patient has a long-standing history of hypertension and diabetes, to avoid any postoperative adrenal crises.
Keyword
MeSH Terms
Figure
-

Fig. 1 Abdominal computed tomography findings. A 2.5×2.0-cm well-circumscribed and homogeneous mass with a density of 60.4 Hounsfield units is seen at the right adrenal gland (arrow).
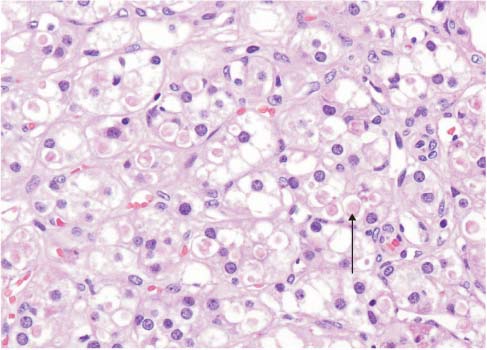
Fig. 2 Photomicrograph of the tumor cells. Clear, vacuolated cytoplasm is admixed with abundant and eosinophilic cytoplasm, which contains spironolactone bodies (arrow; H&E, ×400).
Reference
-
1. Tsagarakis S, Vassiliadi D, Thalassinos N. Endogenous subclinical hypercortisolism: Diagnostic uncertainties and clinical implications. J Endocrinol Invest. 2006; 29:471–482.2. Oh JY. How to approach and follow adrenal incidentaloma? Korean J Intern Med. 2013; 28:541–543.3. Kim BY, Chun AR, Kim KJ, Jung CH, Kang SK, Mok JO, et al. Clinical Characteristics and Metabolic Features of Patients with Adrenal Incidentalomas with or without Subclinical Cushing's Syndrome. Endocrinol Metab (Seoul). 2014; 29:457–463.4. Yoon V, Heyliger A, Maekawa T, Sasano H, Carrick K, Woodruff S, et al. Benign adrenal adenomas secreting excess mineralocorticoids and glucocorticoids. Endocrinol Diabetes Metab Case Rep. 2013; 2013:130042.5. Nieman LK, Biller BM, Findling JW, Newell-Price J, Savage MO, Stewart PM, et al. The diagnosis of Cushing's syndrome: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2008; 93:1526–1540.6. Lenders JW, Duh QY, Eisenhofer G, Gimenez-Roqueplo AP, Grebe SK, Murad MH, et al. Pheochromocytoma and paraganglioma: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2014; 99:1915–1942.7. Young WF, Stanson AW, Thompson GB, Grant CS, Farley DR, van Heerden JA. Role for adrenal venous sampling in primary aldosteronism. Surgery. 2004; 136:1227–1235.8. Funder JW, Carey RM, Fardella C, Gomez-Sanchez CE, Mantero F, Stowasser M, et al. Case detection, diagnosis, and treatment of patients with primary aldosteronism: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2008; 93:3266–3281.9. Patel KA, Calomeni EP, Nadasdy T, Zynger DL. Adrenal gland inclusions in patients treated with aldosterone antagonists (Spironolactone/Eplerenone): incidence, morphology, and ultrastructural findings. Diagn Pathol. 2014; 9:147.10. Aubert S, Wacrenier A, Leroy X, Devos P, Carnaille B, Proye C, et al. Weiss system revisited: a clinicopathologic and immunohistochemical study of 49 adrenocortical tumors. Am J Surg Pathol. 2002; 26:1612–1619.11. Chang KY, Ryu S, Cho JY, Kim HW. Aldosterone- and cortisol-coproducing adrenal adenoma without clinical features of Cushing syndrome. Korean J Intern Med. 2014; 29:679–682.12. Spath M, Korovkin S, Antke C, Anlauf M, Willenberg HS. Aldosterone-and cortisol-co-secreting adrenal tumors: the lost subtype of primary aldosteronism. Eur J Endocrinol. 2011; 164:447–455.13. Lau JH, Sze WC, Reznek RH, Matson M, Sahdev A, Carpenter R, et al. A prospective evaluation of postural stimulation testing, computed tomography and adrenal vein sampling in the differential diagnosis of primary aldosteronism. Clin Endocrinol (Oxf). 2012; 76:182–188.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Periodic Paralysis Due to Aldosterone Producing Adrenal Cortical Adenoma
- A case of idiopathic hyperaldosteronism vs. bilateral aldosterone producing adenoma
- Aldosterone- and cortisol-co-producing adrenal adenoma without clinical features of Cushing syndrome
- A case of adrenocortical adenoma with primary hyperaldosteronism and subclinical Cushing's syndrome
- Bilateral Adrenocortical Masses Producing Aldosterone and Cortisol Independently
