Amiodarone-Induced Pulmonary Toxicity: Percutaneous Needle Aspiration Biopsy and Ultrastructural Findings
- Affiliations
-
- 1Department of Internal Medicine, Ewha Womans University School of Medicine, Seoul, Korea. pseongh@ewha.ac.kr
- 2Department of Pathology, Ewha Womans University School of Medicine, Seoul, Korea.
- KMID: 2171250
- DOI: http://doi.org/10.12771/emj.2013.36.2.144
Abstract
- Amiodarone has been widely used for supraventricular and ventricular arrhythmias and many patients benefit from its effectiveness in treating potentially life-threatening arrhythmias. However, this drug can cause multi-organ toxicity, including amiodarone-induced pulmonary toxicity (APT). Not only does amiodarone have a long half-life but also is lipophilic and therefore can easily accumulate in tissues. Hence, it is difficult to monitor therapeutic levels and side effects, making it difficult to predict toxicities. In this case, we describe multi-organ complications secondary to amiodarone use, especially APT combined with pneumonia with atypical pathogens and pulmonary hemorrhage. The patient reached a high cumulative dose of amiodarone despite a low maintenance dose of amiodarone. This case highlights an unusual presentation of APT with multi-organ toxicity and we review articles regarding the association between the cumulative dose of amiodarone and amiodarone-induced toxicities.
MeSH Terms
Figure
-
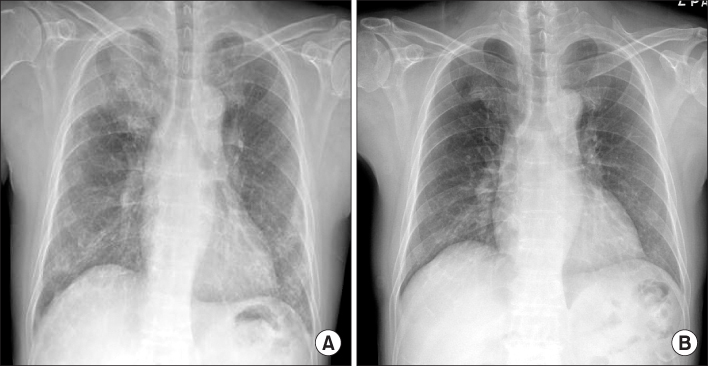
Fig. 1 Chest X-ray showing new right upper lobe consolidation with reticulonodular opacities on both lung fields (A), when compared to a previous chest X-ray (B).
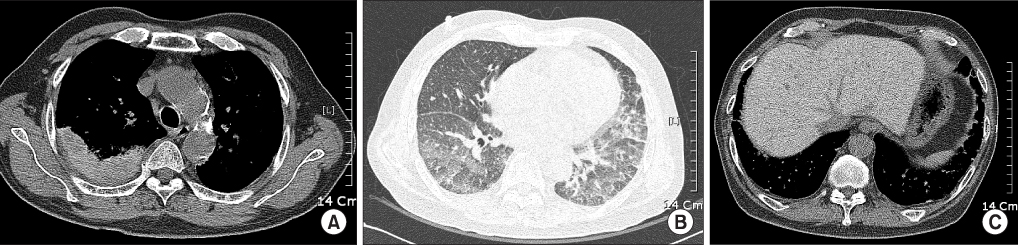
Fig. 2 Chest computed tomography scan showing subpleural consolidation with internal high attenuation (A), subpleural reticular opacity and interlobular septal thickening with patchy ground-glass opacities (B), and diffuse increase in the attenuation of the liver (C).
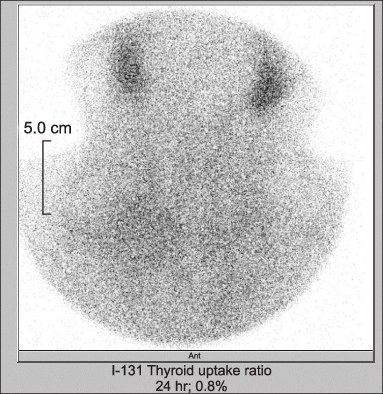
Fig. 3 Thyroid scan showing decreased 24-hour iodine uptake as 0.8%.

Fig. 4 Pathologic analysis of percutaneous needle aspiration biopsy sample showing chronic interstitial inflammation with fibrous thickening of alveolar septum with features of organizing pneumonia (A: H&E, ×200). Some alveolar spaces showing collection of many intra-alveolar foamy macrophages (B: H&E, ×400). A circle shows Oil Red O-positive lipid droplets in the alveolar macrophages.

Fig. 5 Electron micrographs showing the ultrastructures of foamy macrophages with numerous round to oval membrane-bound cytoplasmic inclusions (A, ×10,000). Higher magnification of inclusions showing characteristic, closely spaced concentrically arranged lamellae (B, ×20,000).
Reference
-
1. Stelfox HT, Ahmed SB, Fiskio J, Bates DW. Monitoring amiodarone's toxicities: recommendations, evidence, and clinical practice. Clin Pharmacol Ther. 2004; 75:110–122.2. Jackevicius CA, Tom A, Essebag V, Eisenberg MJ, Rahme E, Tu JV, et al. Population-level incidence and risk factors for pulmonary toxicity associated with amiodarone. Am J Cardiol. 2011; 108:705–710.3. Adams GD, Kehoe R, Lesch M, Glassroth J. Amiodarone-induced pneumonitis: assessment of risk factors and possible risk reduction. Chest. 1988; 93:254–263.4. Jang WJ, Chon HR, Jung JS, Yoo SH, Koh KH, Koh YM, et al. Amiodarone-induced pulmonary toxicity within a short period of the initiation of amiodarone therapy: a case report. Korean J Crit Care Med. 2011; 26:117–121.5. Veltri EP, Reid PR. Amiodarone pulmonary toxicity: early changes in pulmonary function tests during amiodarone rechallenge. J Am Coll Cardiol. 1985; 6:802–805.6. Kerin NZ, Rubenfire M. Detection of amiodarone pulmonary toxicity. J Am Coll Cardiol. 1989; 13:261–262.7. Ernawati DK, Stafford L, Hughes JD. Amiodarone-induced pulmonary toxicity. Br J Clin Pharmacol. 2008; 66:82–87.8. Bouvy ML, Heerdink ER, Hoes AW, Leufkens HG. Amiodarone-induced thyroid dysfunction associated with cumulative dose. Pharmacoepidemiol Drug Saf. 2002; 11:601–606.9. Ashrafian H, Davey P. Is amiodarone an underrecognized cause of acute respiratory failure in the ICU? Chest. 2001; 120:275–282.10. Tanawuttiwat T, Harindhanavudhi T, Hanif S, Sahloul MZ. Amiodarone-induced alveolar haemorrhage: a rare complication of a common medication. Heart Lung Circ. 2010; 19:435–437.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Amiodarone-Induced Pulmonary Toxicity
- Percutaneous Fine Needle Aspiration Biopsy of Lung Masses
- Amiodarone-induced Pulmonary Toxicity within a Short Period of the Initiation of Amiodarone Therapy: A Case Report
- Bronchoalveolar Lavage (BAL) Cytology and Ultrastructural Findings in a Patient with Amiodarone-Induced Pulmonary Toxicity: A Case Report
- A Case of Amiodarone-Induced Pulmonary Toxicity After a Long Course of a Low Dose Therapy
