A Case of Influenza Associated Fulminant Myocarditis Successfully Treated with Intravenous Peramivir
- Affiliations
-
- 1Division of Infectious Diseases, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea. macropha@korea.ac.kr
- 2Department of Biomedical Sciences, Korea University College of Medicine, Seoul, Korea.
- 3Institute of Emerging Infectious Diseases, Korea University College of Medicine, Seoul, Korea.
- KMID: 2170507
- DOI: http://doi.org/10.3947/ic.2015.47.4.272
Abstract
- We report the case of a patient with fulminant myocarditis caused by influenza A virus, who presented with acute-onset heart failure and cardiogenic shock and was treated successfully with single dose of intravenous peramivir and with pharmacologic hemodynamic support. A 45-year-old Korean woman presented to our emergency department (ED) with shortness of breath and an episode of seizure that developed abruptly 5 hours before she arrived in the ED. She had a history of recurrent epileptic seizure 25 years ago, but denied other specific medical illnesses. In the ED, she was hypoxemic (arterial partial pressure of oxygen, 59.8 mmHg on room air) and chest radiography revealed bilateral alveolar infiltrates. A rapid antigen test for influenza A virus was positive, and she was administered a single dose of peramivir (300 mg) intravenously. Five hours later, the patient's dyspnea had worsened and she was hypotensive (blood pressure, 86/53 mmHg), requiring norepinephrine infusion. Further evaluation disclosed an increased cardiac troponin I level of 1.36 ng/mL and a depressed left ventricular ejection fraction of 30%. Under the diagnosis of influenza A-associated myocarditis and cardiogenic shock, she was managed with continuous critical care in the intensive care unit. On day 3, the patient's dyspnea began to resolve and her ventricular function returned to normal. Real-time polymerase chain reaction assays for influenza viruses in serial nasopharyngeal aspirates were positive for influenza A (hH3N2) with a threshold cycle value of 27.39 on day 2, but these became negative by day 4. The patient recovered and was discharged on day 9 after admission. In conclusion, this case indicates that intravenous peramivir might be an effective antiviral agent for the treatment of severe influenza A virus infection.
Keyword
MeSH Terms
-
Critical Care
Diagnosis
Dyspnea
Emergency Service, Hospital
Epilepsy
Female
Heart Failure
Hemodynamics
Humans
Influenza A virus
Influenza, Human*
Intensive Care Units
Middle Aged
Myocarditis*
Norepinephrine
Orthomyxoviridae
Oxygen
Partial Pressure
Radiography
Real-Time Polymerase Chain Reaction
Seizures
Shock, Cardiogenic
Stroke Volume
Thorax
Troponin I
Ventricular Function
Norepinephrine
Oxygen
Troponin I
Figure
-
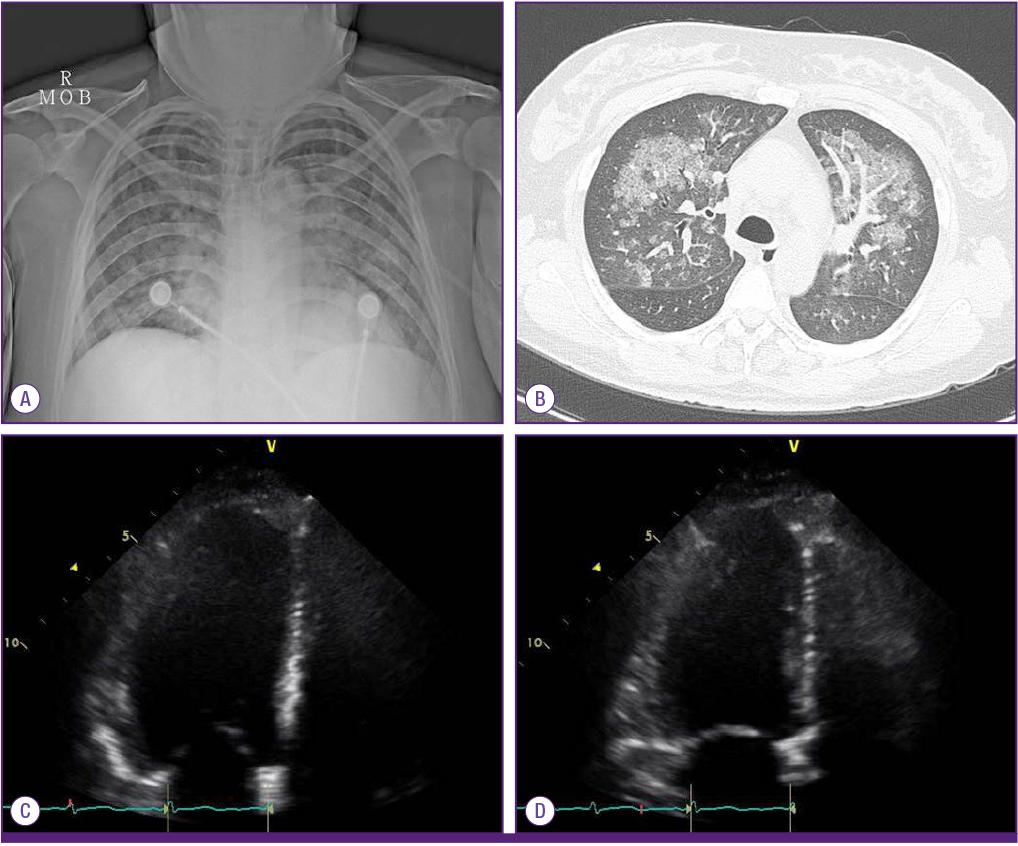
Figure 1 Initial radiologic and echocardiographic findings in a patient with influenza A-associated fulminant myocarditis seen in the emergency department. (A) Chest radiography showing bilateral alveolar infiltrates. (B) Chest computed tomography scan showing bilateral nodular ground-glass opacities and consolidation. (C) Two-dimensional echocardiogram demonstrating diffuse hypokinesia with sparing left ventricular apex in the four-chamber view, end-diastolic phase. (D) End-systolic phase. LA, left atrium; LV, left ventricle.
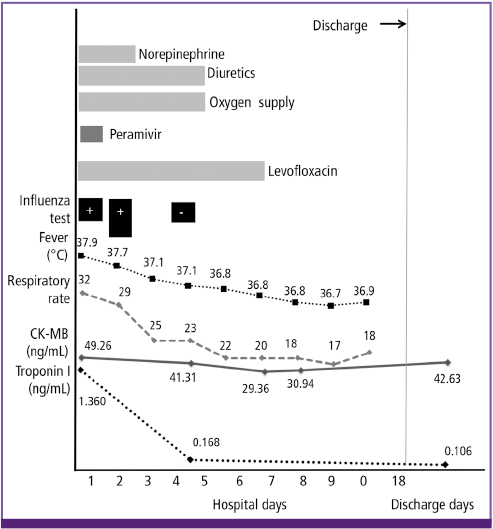
Figure 2 A graph illustrating the clinical course of the influenza-associated fulminant myocarditis case reported in this article, showing changes in clinical findings and supportive measures following the peramivir therapy. RAT, rapid antigen test; RT-PCR, real-time polymerase chain reaction; CK-MB, creatine kinase-myocardial band.
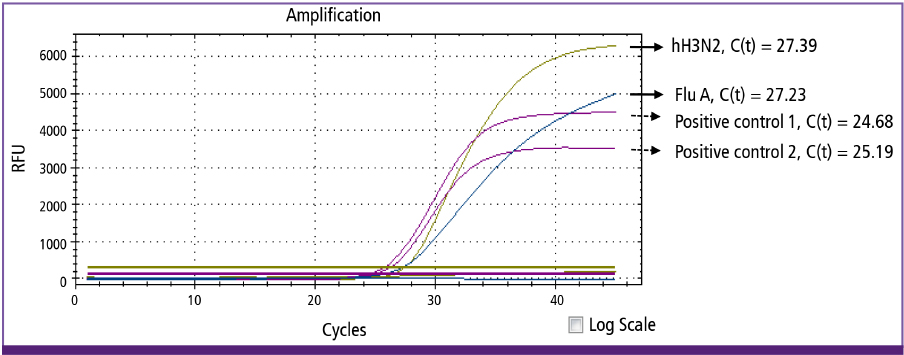
Figure 3 Results of real-time polymerase chain reaction assays showing amplification curves of the influenza A virus and hH3N2 subtype detection on a nasopharyngeal aspirates collected on day 2 of hospitalization. Two positive control samples for human RNase P were included in the assays. RFU, relative fluorescence units; C(t), cycle threshold; Flu A, influenza A.
Reference
-
1. World Health Organization (WHO). Vaccines against influenza WHO position paper - November 2012. Wkly Epidemiol Rec. 2012; 87:461–476.2. Kuiken T, Taubenberger JK. Pathology of human influenza revisited. Vaccine. 2008; 26:Suppl 4. D59–D66.
Article3. Estabragh ZR, Mamas MA. The cardiovascular manifestations of influenza: a systematic review. Int J Cardiol. 2013; 167:2397–2403.
Article4. Birnkrant D, Cox E. The emergency use authorization of peramivir for treatment of 2009 H1N1 influenza. N Engl J Med. 2009; 361:2204–2207.
Article5. Moore DL, Vaudry W, Scheifele DW, Halperin SA, Déry P, Ford-Jones E, Arishi HM, Law BJ, Lebel M, Le Saux N, Grimsrud K, Tam T. Surveillance for influenza admissions among children hospitalized in Canadian immunization monitoring program active centers, 2003-2004. Pediatrics. 2006; 118:e610–e619.
Article6. Gupta S, Markham DW, Drazner MH, Mammen PP. Fulminant myocarditis. Nat Clin Pract Cardiovasc Med. 2008; 5:693–706.
Article7. Ukimura A, Satomi H, Ooi Y, Kanzaki Y. Myocarditis associated with influenza A H1N1pdm2009. Influenza Res Treat. 2012; 2012:351979.
Article8. Yoshimizu N, Tominaga T, Ito T, Nishida Y, Wada Y, Sohmiya K, Tanaka S, Shibata K, Kanzaki Y, Ukimura A, Morita H, Hoshiga M, Ishizaka N. Repetitive fulminant influenza myocarditis requiring the use of circulatory assist devices. Intern Med. 2014; 53:109–114.
Article9. Rogers VL, Sheffield JS, Roberts SW, McIntire DD, Luby JP, Trevino S, Wendel GD Jr. Presentation of seasonal influenza A in pregnancy: 2003-2004 influenza season. Obstet Gynecol. 2010; 115:924–929.10. Ando M, Miyazaki E, Hiroshige S, Ashihara Y, Okubo T, Ueo M, Fukami T, Sugisaki K, Tsuda T, Ohishi K, Yoshitake S, Noguchi T, Kumamoto T. Virus associated hemophagocytic syndrome accompanied by acute respiratory failure caused by influenza A (H3N2). Intern Med. 2006; 45:1183–1186.
Article11. Nolte KB, Alakija P, Oty G, Shaw MW, Subbarao K, Guarner J, Shieh WJ, Dawson JE, Morken T, Cox NJ, Zaki SR. Influenza A virus infection complicated by fatal myocarditis. Am J Forensic Med Pathol. 2000; 21:375–379.
Article12. Ison MG, Fraiz J, Heller B, Jauregui L, Mills G, O'Riordan W, O'Neil B, Playford EG, Rolf JD, Sada-Diaz E, Elder J, Collis P, Hernandez JE, Sheridan WP. Intravenous peramivir for treatment of influenza in hospitalized patients. Antivir Ther. 2014; 19:349–361.
Article13. Hernandez JE, Adiga R, Armstrong R, Bazan J, Bonilla H, Bradley J, Dretler R, Ison MG, Mangino JE, Maroushek S, Shetty AK, Wald A, Ziebold C, Elder J, Hollister AS, Sheridan W. eIND Peramivir Investigators. Clinical experience in adults and children treated with intravenous peramivir for 2009 influenza A (H1N1) under an Emergency IND program in the United States. Clin Infect Dis. 2011; 52:695–706.
Article14. Cobas M, Abbo L, Santos M, Baccini-Jauregui C, Pham S. Successful management of fulminant influenza A subtype H1N1 myocarditis. BMJ Case Rep. 2010; 2010:pii: bcr0220102763.
Article15. Biocryst Pharmaceuticals. Rapivab (peramivir injection) package insert. 2014. Accessed 25 April 2015. Available at: http://www.rapivab.com/prescribing-information/.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute fulminant myocarditis following influenza vaccination requiring extracorporeal membrane oxygenation
- Comparison of Efficacy of Intravenous Peramivir and Oral Oseltamivir for the Treatment of Influenza: Systematic Review and Meta-Analysis
- Successfully Treated Acute Fulminant Myocarditis Induced by Ulcerative Colitis with Extracorporeal Life Support and Infliximab
- A Case of Acute Fulminant Myocarditis Progressed into and Recovered from Congestive Heart Failure and Multiorgan Failure
- Percutaneous Extracorporeal Membrane Oxygenation (ECMO) for Acute Fulminant Myocarditis
