Infect Chemother.
2011 Feb;43(1):60-63. 10.3947/ic.2011.43.1.60.
A Case of Fournier's Gangrene Caused by Streptococcus anginosus
- Affiliations
-
- 1Department of Internal Medicine, Seoul Medical Center, Seoul, Korea. dasole@seoulmc.or.kr
- 2Department of Laboratory Medicine, Seoul Medical Center, Seoul, Korea.
- 3Department of Urology, Seoul Medical Center, Seoul, Korea.
- KMID: 2170335
- DOI: http://doi.org/10.3947/ic.2011.43.1.60
Abstract
- Fournier's gangrene is a rare, rapidly progressive, necrotizing fasciitis of the genital, perianal and perineal regions. It is usually caused by a synergistic infection of aerobic and anaerobic organisms. A 51-year-old male patient with diabetes mellitus and chronic renal insufficiency on peritoneal dialysis was admitted with severe scrotal pain and swelling that lasted 4 days. An emergent non-contrast-enhanced computed tomography revealed extensive gas formation, fatty haziness and edema in the left scrotal and inguinal area. The patient was successfully treated with immediate surgical debridements and antibiotics. Streptococcus anginosus group Streptococcus anginosus was isolated from surgical wound cultures and identified with biochemical identification methods and direct sequencing of DNA. Herein, we report a rare case of Fournier's gangrene caused by S. anginosus. We also review the relevant literature
MeSH Terms
Figure
-

Figure 1 Non-contrast enhanced computed tomography shows multiple air-bubbles, fatty haziness and swelling in the left scrotum and inguinal area.

Figure 2 Pinpoint white colonies with β-hemolysis are seen on the blood agar plate after 24 hours of incubation.
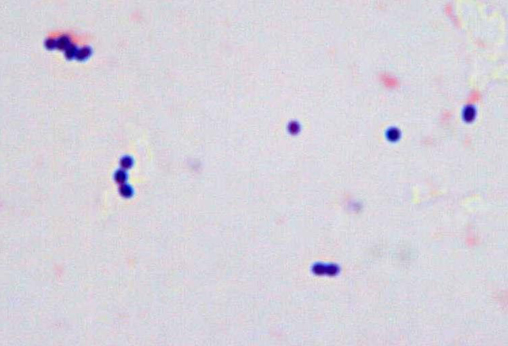
Figure 3 Microscopy shows Gram positive cocci in pairs or short chains (Gram stain, ×1,000).
Reference
-
1. Morpurgo E, Galandiuk S. Fournier's gangrene. Surg Clin North Am. 2002. 82:1213–1224.
Article2. Smith GL, Bunker CB, Dinneen MD. Fournier's gangrene. Br J Urol. 1998. 81:347–355.
Article3. Eke N. Fournier's gangrene: a review of 1726 cases. Br J Surg. 2000. 87:718–728.
Article4. Sorensen MD, Krieger JN, Rivara FP, Broghammer JA, Klein MB, Mack CD, Wessells H. Fournier's Gangrene: population based epidemiology and outcomes. J Urol. 2009. 181:2120–2126.
Article5. Paty R, Smith AD. Gangrene and Fournier's gangrene. Urol Clin North Am. 1992. 19:149–162.
Article6. Norton KS, Johnson LW, Perry T, Perry KH, Sehon JK, Zibari GB. Management of Fournier's gangrene: an eleven year retrospective analysis of early recognition, diagnosis, and treatment. Am Surg. 2002. 68:709–713.7. Uluğ M, Gedik E, Girgin S, Celen MK, Ayaz C. The evaluation of microbiology and Fournier's gangrene severity index in 27 patients. Int J Infect Dis. 2009. 13:e424–e430.
Article8. Kuo CF, Wang WS, Lee CM, Liu CP, Tseng HK. Fournier's gangrene: ten-year experience in a medical center in northern Taiwan. J Microbiol Immunol Infect. 2007. 40:500–506.9. Kim BH, Chang HS, Park CH, Kim CI, Kim KS. Necessity of aggressive management in Fournier's gangrene. Korean J Urol. 2004. 45:793–799.10. Kim SK, Park JI, Joo YT, Park ST, Ha WS, Hong SC, Lee YJ, Jung EJ, Jeung CY, Choi SK. Fournier's gangrene: clinical analysis of 11 patients. J Korean Surg Soc. 2006. 71:274–279.11. Lim SD, Lee SJ, Jeong HJ. The study of prognostic factors in fournier's gangrenes. Korean J Urol. 2002. 43:412–417.12. Piscitelli SC, Shwed J, Schreckenberger P, Danziger LH. Streptococcus milleri group: renewed interest in an elusive pathogen. Eur J Clin Microbiol Infect Dis. 1992. 11:491–498.13. Whiley RA, Beighton D, Winstanley TG, Fraser HY, Hardie JM. Streptococcus intermedius, Streptococcus constellatus, and Streptococcus anginosus (the Streptococcus milleri group): association with different body sites and clinical infections. J Clin Microbiol. 1992. 30:243–244.
Article14. Claridge JE 3rd, Attorri S, Musher DM, Hebert J, Dunbar S. Streptococcus intermedius, Streptococcus constellatus, and Streptococcus anginosus ("Streptococcus milleri group") are of different clinical importance and are not equally associated with abscess. Clin Infect Dis. 2001. 32:1511–1515.15. Han WJ, Cho MS, Lee JH, Ahn HD, Yoon KH, Seo JG, Kim JY, Kim SY, Park YS, Seo YH, Cho YK. A case of humeral osteomyelitis and soft tissue abscess accompanied with Streptococcus anginosus bacteremia. Infect Chemother. 2008. 40:281–283.
Article16. Bantar C, Fernandez Canigia L, Relloso S, Lanza A, Bianchini H, Smayevsky J. Species belonging to the "Streptococcus milleri" group: antimicrobial susceptibility and comparative prevalence in significant clinical specimens. J Clin Microbiol. 1996. 34:2020–2022.
Article17. Tracy M, Wanahita A, Shuhatovich Y, Goldsmith EA, Clarridge JE 3rd, Musher DM. Antibiotic susceptibilities of genetically characterized Streptococcus milleri group strains. Antimicrob Agents Chemother. 2001. 45:1511–1514.
Article18. Levenson RB, Singh AK, Novelline RA. Fournier gangrene: role of imaging. Radiographics. 2008. 28:519–528.
Article
