Endocrinol Metab.
2011 Sep;26(3):253-257. 10.3803/EnM.2011.26.3.253.
A Case of Primary Adrenal Insufficiency in a Patient with Acquired Immunodeficiency Syndrome
- Affiliations
-
- 1Department of Endocrinology and Metabolism, College of Medicine, Kyung Hee University, Seoul, Korea. jik1016@khu.ac.kr
- 2Department of Infection, College of Medicine, Kyung Hee University, Seoul, Korea.
- KMID: 2169178
- DOI: http://doi.org/10.3803/EnM.2011.26.3.253
Abstract
- The adrenal gland is the most commonly involved endocrine organ in patients infected with the human immunodeficiency virus (HIV). Adrenal function abnormality is more common in HIV patients than in the general population. It is important to recognize the condition of adrenal insufficiency, as this adrenal disorder may prove fatal if left untreated. Herein, we report a case of primary adrenal insufficiency in a 37-year-old male patient with acquired immunodeficiency syndrome. The patient complained of fever, general weakness, and fatigue. Impaired adrenal function was noted in the rapid ACTH stimulation test. After steroid supplementation, the patient's symptoms were improved. Therefore, HIV care physicians should ascertain adrenal dysfunction in HIV patients when they complain of fever and general weakness.
MeSH Terms
Figure
-

Fig. 1 Abdominal CT scan showed normal contour of right (A, C) and left (B, C) adrenal glands (arrows).
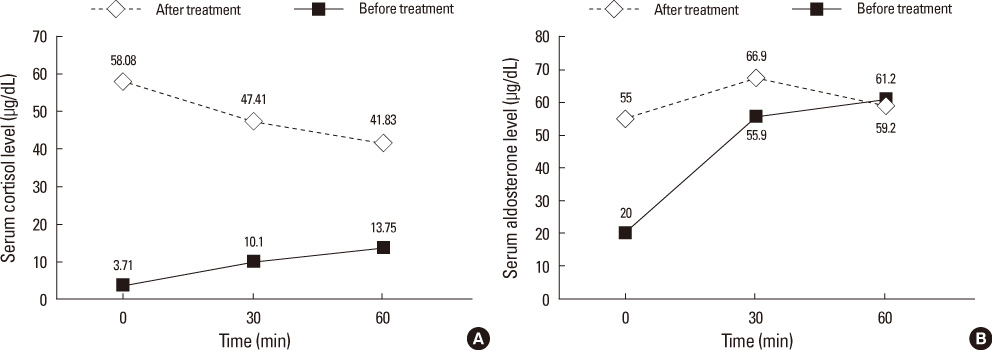
Fig. 2 The results of rapid ACTH stimulation test before and after cortisol replacement therapy. A. Cortisol response after ACTH stimulation was abnormal because the peak cortisol level was less than 18 µg/mL. B. The increased gap of aldosterone after ACTH stimulation was less than 50 pg/mL which suggested decreased response of aldosterone.
Reference
-
1. Aron DC. Endocrine complications of the acquired immunodeficiency syndrome. Arch Intern Med. 1989. 149:330–333.2. Masharani U, Schambelan M. The endocrine complications of acquired immunodeficiency syndrome. Adv Intern Med. 1993. 38:323–336.3. McKee JI, Finlay WEI. Cortisol replacement in severely stressed patients. Lancet. 1983. 321:484.4. Reichert CM, O'Leary TJ, Levens DL, Simrell CR, Macher AM. Autopsy pathology in the acquired immune deficiency syndrome. Am J Pathol. 1983. 112:357–382.5. Glasgow BJ, Steinsapir KD, Anders K, Layfield LJ. Adrenal pathology in the acquired immune deficiency syndrome. Am J Clin Pathol. 1985. 84:594–597.6. Bricaire F, Marche C, Zoubi D, Regnier B, Saimot AG. Adrenocortical lesions and AIDS. Lancet. 1988. 331:881.7. Dobs AS, Dempsey MA, Ladenson PW, Polk BF. Endocrine disorders in men infected with human immunodeficiency virus. Am J Med. 1988. 84:611–616.8. Merenich JA, McDermott MT, Asp AA, Harrison SM, Kidd GS. Evidence of endocrine involvement early in the course of human immunodeficiency virus infection. J Clin Endocrinol Metab. 1990. 70:566–571.9. Findling JW, Buggy BP, Gilson IH, Brummitt CF, Bernstein BM, Raff H. Longitudinal evaluation of adrenocortical function in patients infected with the human immunodeficiency virus. J Clin Endocrinol Metab. 1994. 79:1091–1096.10. Zapanti E, Terzidis K, Chrousos G. Dysfunction of the hypothalamic-pituitary-adrenal axis in HIV infection and disease. Hormones (Athens). 2008. 7:205–216.11. Pulakhandam U, Dincsoy HP. Cytomegaloviral adrenalitis and adrenal insufficiency in AIDS. Am J Clin Pathol. 1990. 93:651–656.12. Sonino N. The use of ketoconazole as an inhibitor of steroid production. N Engl J Med. 1987. 317:812–818.13. Leinung MC, Liporace R, Miller CH. Induction of adrenal suppression by megestrol acetate in patients with AIDS. Ann Intern Med. 1995. 122:843–845.14. Merrill JE, Koyanagi Y, Chen IS. Interleukin-1 and tumor necrosis factor alpha can be induced from mononuclear phagocytes by human immunodeficiency virus type 1 binding to the CD4 receptor. J Virol. 1989. 63:4404–4408.15. Gaillard RC, Turnill D, Sappino P, Muller AF. Tumor necrosis factor alpha inhibits the hormonal response of the pituitary gland to hypothalamic releasing factors. Endocrinology. 1990. 127:101–106.16. Salim YS, Faber V, Wiik A, Andersen PL, Hoier-Madsen M, Mouritsen S. Anti-corticosteroid antibodies in AIDS patients. APMIS. 1988. 96:889–894.17. Werbel SS, Ober KP. Acute adrenal insufficiency. Endocrinol Metab Clin North Am. 1993. 22:303–328.18. Eledrisi MS, Verghese AC. Adrenal insufficiency in HIV infection: a review and recommendations. Am J Med Sci. 2001. 321:137–144.19. Prasanthai V, Sunthornyothin S, Phowthongkum P, Suankratay C. Prevalence of adrenal insufficiency in critically ill patients with AIDS. J Med Assoc Thai. 2007. 90:1768–1774.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Primary Adrenal Insufficiency Presenting as the Initial Clinical Manifestation of Primary Antiphospholipid Antibody Syndrome
- Cutaneous Cytomegalovirus Infection Presenting as Papules and Pustules in a Patient with Acquired Immunodeficiency Syndrome
- A Case of Molluscum Contagiosum in an AIDS Patient
- Ocular Findings in the Acquired Immunodeficiency Syndrome
- A Case of Urethral Diverticulo-Rectal Fistula in Acquired Immunodeficiency Syndrome
