Ann Surg Treat Res.
2015 Apr;88(4):208-214. 10.4174/astr.2015.88.4.208.
Follow-up results of acute portal and splenic vein thrombosis with or without anticoagulation therapy after hepatobiliary and pancreatic surgery
- Affiliations
-
- 1Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. yjpark1974@gmail.com
- KMID: 2167017
- DOI: http://doi.org/10.4174/astr.2015.88.4.208
Abstract
- PURPOSE
Acute portal and splenic vein thrombosis (APSVT) after hepatobiliary and pancreatic (HBP) surgery is a rare but serious complication and a treatment strategy has not been well established. To assess the safety and efficacy of anticoagulation therapy for treating APSVT after HBP surgery.
METHODS
We performed a retrospective case-control study of 82 patients who were diagnosed with APSVT within 4 weeks after HBP surgery from October 2002 to November 2012 at a single institute. We assigned patients to the anticoagulation group (n = 32) or nonanticoagulation group (n = 50) and compared patient characteristics, complications, and the recanalization rate of APSVT between these two groups.
RESULTS
APSVT was diagnosed a mean of 8.6 +/- 4.8 days after HBP surgery. Patients' characteristics were not significantly different between the two groups. There were no bleeding complications related to anticoagulation therapy. The 1-year cumulative recanalization rate of anticoagulation group and nonanticoagulation group were 71.4% and 34.1%, respectively, which is statistically significant (log-rank test, P = 0.0001). In Cox regression model for multivariate analysis, independent factors associated with the recanalization rate of APSVT after HBP surgery were anticoagulation therapy (P = 0.003; hazard ration [HR], 2.364; 95% confidence interval [CI], 1.341-4.168), the absence of a vein reconstruction procedure (P = 0.027; HR, 2.557; 95% CI, 1.111-5.885), and operation type (liver resection rather than pancreatic resection; P = 0.005, HR, 2.350; 95% CI, 1.286-4.296).
CONCLUSION
Anticoagulation therapy appears to be a safe and effective treatment for patients with APSVT after HBP surgery. Further prospective studies of larger patient populations are necessary to confirm our findings.
Keyword
MeSH Terms
Figure
-
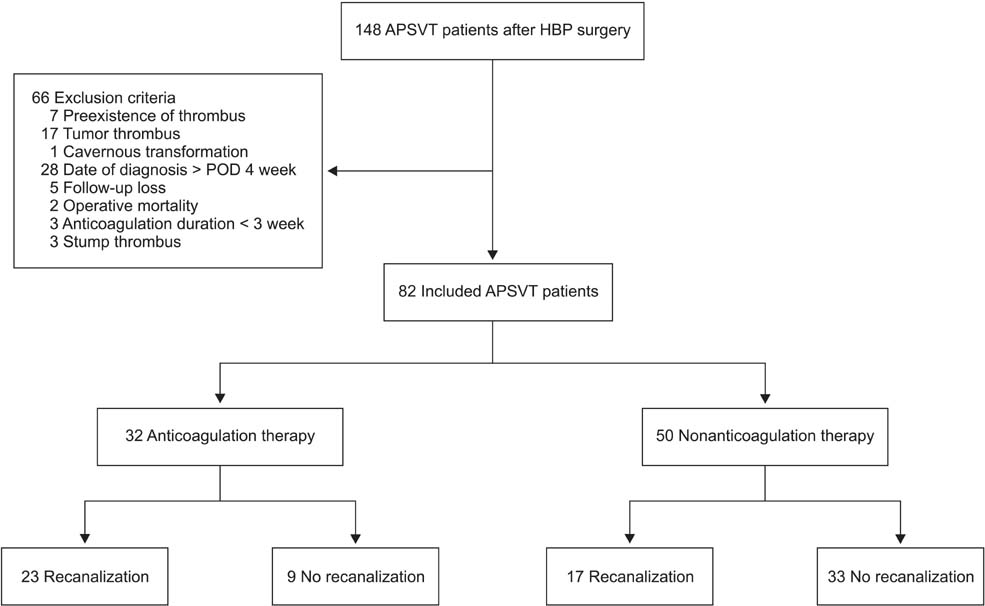
Fig. 1 Study design and outcomes of anticoagulation and no anticoagulation group. APSVT, acute portal and splenic vein thrombosis; HBP, hepatobiliary and pancreatic; POD, postoperative day.
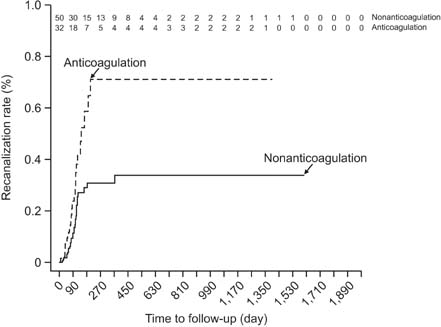
Fig. 2 A significant association between recanalization rate and anticoagulation in multivariate Cox-regression model (P = 0.003; hazard ratio, 2.364; 95% confidence interval, 1.341-4.168).
Reference
-
1. Janssen HL, Wijnhoud A, Haagsma EB, van Uum SH, van Nieuwkerk CM, Adang RP, et al. Extrahepatic portal vein thrombosis: aetiology and determinants of survival. Gut. 2001; 49:720–724.2. Smoot RL, Christein JD, Farnell MB. Durability of portal venous reconstruction following resection during pancreaticoduodenectomy. J Gastrointest Surg. 2006; 10:1371–1375.3. Thomas RM, Ahmad SA. Management of acute post-operative portal venous thrombosis. J Gastrointest Surg. 2010; 14:570–577.4. Kumar S, Sarr MG, Kamath PS. Mesenteric venous thrombosis. N Engl J Med. 2001; 345:1683–1688.5. Plessier A, Darwish-Murad S, Hernandez-Guerra M, Consigny Y, Fabris F, Trebicka J, et al. Acute portal vein thrombosis unrelated to cirrhosis: a prospective multicenter follow-up study. Hepatology. 2010; 51:210–218.6. Tublin ME, Dodd GD 3rd, Baron RL. Benign and malignant portal vein thrombosis: differentiation by CT characteristics. AJR Am J Roentgenol. 1997; 168:719–723.7. Yerdel MA, Gunson B, Mirza D, Karayalçin K, Olliff S, Buckels J, et al. Portal vein thrombosis in adults undergoing liver transplantation: risk factors, screening, management, and outcome. Transplantation. 2000; 69:1873–1881.8. Reddy SK, Barbas AS, Turley RS, Steel JL, Tsung A, Marsh JW, et al. A standard definition of major hepatectomy: resection of four or more liver segments. HPB (Oxford). 2011; 13:494–502.9. Snipelisky D, Kusumoto F. Current strategies to minimize the bleeding risk of warfarin. J Blood Med. 2013; 4:89–99.10. Lip GY, Andreotti F, Fauchier L, Huber K, Hylek E, Knight E, et al. Bleeding risk assessment and management in atrial fibrillation patients: a position document from the European Heart Rhythm Association, endorsed by the European Society of Cardiology Working Group on Thrombosis. Europace. 2011; 13:723–746.11. DiMarco JP, Flaker G, Waldo AL, Corley SD, Greene HL, Safford RE, et al. Factors affecting bleeding risk during anticoagulant therapy in patients with atrial fibrillation: observations from the Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) study. Am Heart J. 2005; 149:650–656.12. Condat B, Pessione F, Hillaire S, Denninger MH, Guillin MC, Poliquin M, et al. Current outcome of portal vein thrombosis in adults: risk and benefit of anticoagulant therapy. Gastroenterology. 2001; 120:490–497.13. Holbrook AM, Pereira JA, Labiris R, McDonald H, Douketis JD, Crowther M, et al. Systematic overview of warfarin and its drug and food interactions. Arch Intern Med. 2005; 165:1095–1106.14. Palareti G, Cosmi B. Bleeding with anticoagulation therapy: who is at risk, and how best to identify such patients. Thromb Haemost. 2009; 102:268–278.15. Condat B, Pessione F, Helene Denninger M, Hillaire S, Valla D. Recent portal or mesenteric venous thrombosis: increased recognition and frequent recanalization on anticoagulant therapy. Hepatology. 2000; 32:466–470.16. Demertzis S, Ringe B, Gulba D, Rosenthal H, Pichlmayr R. Treatment of portal vein thrombosis by thrombectomy and regional thrombolysis. Surgery. 1994; 115:389–393.17. Klempnauer J, Grothues F, Bektas H, Pichlmayr R. Results of portal thrombectomy and splanchnic thrombolysis for the surgical management of acute mesentericoportal thrombosis. Br J Surg. 1997; 84:129–132.18. Zyromski NJ, Howard TJ. Acute superior mesenteric-portal vein thrombosis after pancreaticoduodenectomy: treatment by operative thrombectomy. Surgery. 2008; 143:566–567.19. Henao EA, Bohannon WT, Silva MB Jr. Treatment of portal venous thrombosis with selective superior mesenteric artery infusion of recombinant tissue plasminogen activator. J Vasc Surg. 2003; 38:1411–1415.20. Malkowski P, Pawlak J, Michalowicz B, Szczerban J, Wroblewski T, Leowska E, et al. Thrombolytic treatment of portal thrombosis. Hepatogastroenterology. 2003; 50:2098–2100.21. Ozkan U, Oguzkurt L, Tercan F, Tokmak N. Percutaneous transhepatic thrombolysis in the treatment of acute portal venous thrombosis. Diagn Interv Radiol. 2006; 12:105–107.22. Kaplan JL, Weintraub SL, Hunt JP, Gonzalez A, Lopera J, Brazzini A. Treatment of superior mesenteric and portal vein thrombosis with direct thrombolytic infusion via an operatively placed mesenteric catheter. Am Surg. 2004; 70:600–604.23. Tseng JF, Raut CP, Lee JE, Pisters PW, Vauthey JN, Abdalla EK, et al. Pancreaticoduodenectomy with vascular resection: margin status and survival duration. J Gastrointest Surg. 2004; 8:935–949.24. Garcia-Pagan JC, Hernandez-Guerra M, Bosch J. Extrahepatic portal vein thrombosis. Semin Liver Dis. 2008; 28:282–292.25. Sobhonslidsuk A, Reddy KR. Portal vein thrombosis: a concise review. Am J Gastroenterol. 2002; 97:535–541.26. Ouaissi M, Sielezneff I, Pirro N, Bon Mardion R, Chaix JB, Merad A, et al. Therapeutic anticoagulant does not modify thromboses rate vein after venous reconstruction following pancreaticoduodenectomy. Gastroenterol Res Pract. 2008; 2008:896320.27. Carrere N, Sauvanet A, Goere D, Kianmanesh R, Vullierme MP, Couvelard A, et al. Pancreaticoduodenectomy with mesentericoportal vein resection for adenocarcinoma of the pancreatic head. World J Surg. 2006; 30:1526–1535.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Isolated Splenic Vein Thrombosis Associated with Acute Pancreatitis
- Portal and Splenic Vein Thrombosis Successfully Treated with Anticoagulants in Acute Pancreatitis
- Nephrotic syndrome complicated with portal, splenic, and superior mesenteric vein thrombosis
- A Case of Isolated Superior Mesenteric Vein Thrombosis in Acute Pancreatitis
- Non-invasive MR Demonstration of the Fistula between Pancreatic Pseudocyst and Portal Vein: A Case Report
