Clinical Concerns about Recurrence of Non-Functioning Pituitary Adenoma
- Affiliations
-
- 1Department of Neurosurgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. nsnam@skku.edu
- 2Department of Neurosurgery, Konyang University Hospital, Seoul, Korea.
- KMID: 2165226
- DOI: http://doi.org/10.14791/btrt.2016.4.1.1
Abstract
- BACKGROUND
Non-functioning pituitary adenomas (NFPA) are clinically challenging because they present at a late stage with local mass effects or hypopituitarism. Surgery for non-functioning pituitary adenoma requires a special strategic approach for both minimal morbidity and radical resection. However, the clinical predictive factors associated with recurrence are limited. Here, we investigated optimal treatment of non-functioning pituitary adenoma.
METHODS
We enrolled 289 patients who presented with non-functioning pituitary adenoma between January 2000 and January 2012 and who had received follow-up for at least one year for this retrospective study. Of these patients, 152 were male and 137 were female, with a median age of 51 years (range 15.79 years) and a median follow-up of four years (range 1.12.6 years). Characteristics of patients and tumors were reviewed with electronic medical records and radiologic images, retrospectively.
RESULTS
Of the tumors, 193 were gross-totally resected, 53 were near-totally resected, and 43 were sub-totally resected. The extent of resection and adjuvant radiotherapy were both statistically significant prognostic factors of recurrence. Immunohistochemistry of tumor specimens did not yield consistent results.
CONCLUSION
With a high rate of recurrence, NFPA should be closely followed-up over a long-term period. Improvement of surgical techniques with advanced surgical equipment and adjuvant radiosurgery would lead to reduce the recurrence rate and improve patients' outcome.
MeSH Terms
Figure
-
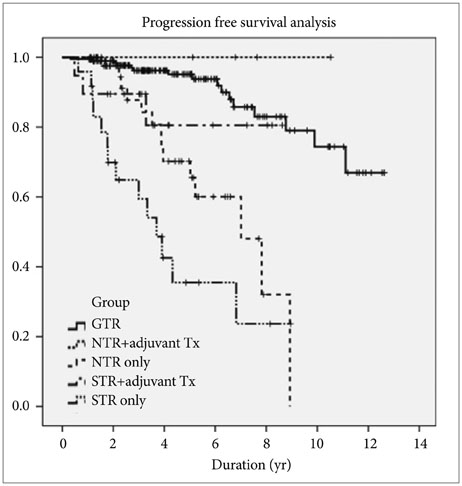
Fig. 1 Progression-free survival between groups based on extent of resection and administration of adjuvant treatment. GTR, gross total removal; NTR, near total removal; STR, subtotal removal; Tx, treatment.
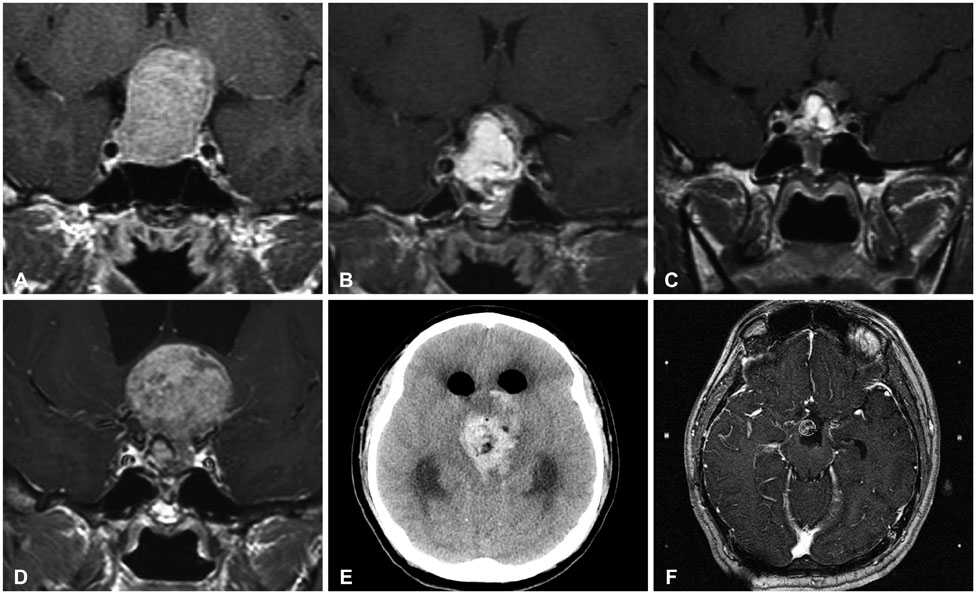
Fig. 2 Illustrative case. A 22-year-old male patient presented with visual field defects. A: Initial MRI showed pituitary adenoma. B: Suspicious residual mass identified after operation. C: 1-yr postoperative MRI showed progression. The patient was lost to follow-up without any further treatment. D: 6-yr postoperative MRI showed significantly progression with hydrocephalus. E: After the second operation, intra-cerebral hemorrhage with intra-ventricular hemorrhage occurred. F: An adjuvant gamma knife radiosurgery was conducted to the residual tumor.
Cited by 1 articles
-
Therapeutic Strategy for Cavernous Sinus-Invading Non-Functioning Pituitary Adenomas Based on the Modified Knosp Grading System
Juyoung Hwang, Ho Jun Seol, Do-Hyun Nam, Jung-Il Lee, Min Ho Lee, Doo-Sik Kong
Brain Tumor Res Treat. 2016;4(2):63-69. doi: 10.14791/btrt.2016.4.2.63.
Reference
-
1. Mortini P, Barzaghi R, Losa M, Boari N, Giovanelli M. Surgical treatment of giant pituitary adenomas: strategies and results in a series of 95 consecutive patients. Neurosurgery. 2007; 60:993–1002. discussion 1003-4.2. Roelfsema F, Biermasz NR, Pereira AM. Clinical factors involved in the recurrence of pituitary adenomas after surgical remission: a structured review and meta-analysis. Pituitary. 2012; 15:71–83.
Article3. Laws ER Jr, Fode NC, Redmond MJ. Transsphenoidal surgery following unsuccessful prior therapy. An assessment of benefits and risks in 158 patients. J Neurosurg. 1985; 63:823–829.4. Farrell WE, Clayton RN. Molecular pathogenesis of pituitary tumors. Front Neuroendocrinol. 2000; 21:174–198.
Article5. Saeger W. Pituitary tumors: prognostic indicators. Endocrine. 2005; 28:57–66.6. Noh TW, Jeong HJ, Lee MK, Kim TS, Kim SH, Lee EJ. Predicting recurrence of nonfunctioning pituitary adenomas. J Clin Endocrinol Metab. 2009; 94:4406–4413.
Article7. Gejman R, Swearingen B, Hedley-Whyte ET. Role of Ki-67 proliferation index and p53 expression in predicting progression of pituitary adenomas. Hum Pathol. 2008; 39:758–766.
Article8. Šteňo A, Bocko J, Rychlý B, et al. Nonfunctioning pituitary adenomas: association of Ki-67 and HMGA-1 labeling indices with residual tumor growth. Acta Neurochir (Wien). 2014; 156:451–461. discussion 461.
Article9. Ferrante E, Ferraroni M, Castrignanò T, et al. Non-functioning pituitary adenoma database: a useful resource to improve the clinical management of pituitary tumors. Eur J Endocrinol. 2006; 155:823–829.
Article10. Boelaert K, Gittoes NJ. Radiotherapy for non-functioning pituitary adenomas. Eur J Endocrinol. 2001; 144:569–575.
Article11. Greenman Y, Ouaknine G, Veshchev I, Reider-Groswasser II, Segev Y, Stern N. Postoperative surveillance of clinically nonfunctioning pituitary macroadenomas: markers of tumour quiescence and regrowth. Clin Endocrinol (Oxf). 2003; 58:763–769.
Article12. Park P, Chandler WF, Barkan AL, et al. The role of radiation therapy after surgical resection of nonfunctional pituitary macroadenomas. Neurosurgery. 2004; 55:100–106. discussion 106-7.
Article13. van den Bergh AC, van den Berg G, Schoorl MA, et al. Immediate postoperative radiotherapy in residual nonfunctioning pituitary adenoma: beneficial effect on local control without additional negative impact on pituitary function and life expectancy. Int J Radiat Oncol Biol Phys. 2007; 67:863–869.
Article14. Erridge SC, Conkey DS, Stockton D, et al. Radiotherapy for pituitary adenomas: long-term efficacy and toxicity. Radiother Oncol. 2009; 93:597–601.
Article15. Gittoes NJ, Bates AS, Tse W, et al. Radiotherapy for non-function pituitary tumours. Clin Endocrinol (Oxf). 1998; 48:331–337.16. Kong DS, Lee JI, Lim DH, et al. The efficacy of fractionated radiotherapy and stereotactic radiosurgery for pituitary adenomas: long-term results of 125 consecutive patients treated in a single institution. Cancer. 2007; 110:854–860.
Article17. van Beek AP, van den Bergh AC, van den Berg LM, et al. Radiotherapy is not associated with reduced quality of life and cognitive function in patients treated for nonfunctioning pituitary adenoma. Int J Radiat Oncol Biol Phys. 2007; 68:986–991.
Article18. Brummelman P, Elderson MF, Dullaart RP, et al. Cognitive functioning in patients treated for nonfunctioning pituitary macroadenoma and the effects of pituitary radiotherapy. Clin Endocrinol (Oxf). 2011; 74:481–487.
Article19. Sattler MG, Meiners LC, Sluiter WJ, et al. Brain abnormalities on MRI in non-functioning pituitary adenoma patients treated with or without postoperative radiotherapy. Radiother Oncol. 2015; 114:239–244.
Article20. Auer LM, Clarici G. The first 100 transsphenoidally operated pituitary adenomas in a non-specialised centre: surgical results and tumour-recurrence. Neurol Res. 1985; 7:153–160.
Article21. Ramm-Pettersen J, Berg-Johnsen J, Hol PK, et al. Intra-operative MRI facilitates tumour resection during trans-sphenoidal surgery for pituitary adenomas. Acta Neurochir (Wien). 2011; 153:1367–1373.
Article22. Goudakos JK, Markou KD, Georgalas C. Endoscopic versus microscopic trans-sphenoidal pituitary surgery: a systematic review and meta-analysis. Clin Otolaryngol. 2011; 36:212–220.
Article23. Strychowsky J, Nayan S, Reddy K, Farrokhyar F, Sommer D. Purely endoscopic transsphenoidal surgery versus traditional microsurgery for resection of pituitary adenomas: systematic review. J Otolaryngol Head Neck Surg. 2011; 40:175–185.24. Rotenberg B, Tam S, Ryu WH, Duggal N. Microscopic versus endoscopic pituitary surgery: a systematic review. Laryngoscope. 2010; 120:1292–1297.
Article25. Yang I, Wang MB, Bergsneider M. Making the transition from microsurgery to endoscopic trans-sphenoidal pituitary neurosurgery. Neurosurg Clin N Am. 2010; (21):643–651. vi.
Article26. Tao Y, Jian-wen G, Yong-qin K, et al. Transsphenoidal surgery assisted by a new guidance device: results of a series of 747 cases. Clin Neurol Neurosurg. 2011; 113:626–630.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Neurosurgical Treatment of Giant Pituitary Adenoma
- Pituitary Apoplexy due to Pituitary Adenoma Infarction
- A Case of Impotence due to Pituitary Adenoma
- Two Cases of Pituitary Hyperplasia Secondary to Primary Hypothyroidism Mimicking Pituitary Tumor
- Pituitary Adenoma Confined Within the Pituitary Stalk: A Case Report and Literature Review
