Korean J Gastroenterol.
2014 Dec;64(6):340-347. 10.4166/kjg.2014.64.6.340.
The Clinical Value of 18F-Fluorodeoxyglucose Uptake on Positron Emission Tomography/Computed Tomography for Predicting Regional Lymph Node Metastasis and Non-curative Surgery in Primary Gastric Carcinoma
- Affiliations
-
- 1Department of Internal Medicine, Ewha Medical Research Institute, Ewha Womans University School of Medicine, Seoul, Korea. shimkn@ewha.ac.kr
- KMID: 2160666
- DOI: http://doi.org/10.4166/kjg.2014.64.6.340
Abstract
- BACKGROUND/AIMS
Accurate preoperative detection of regional lymph nodes and evaluation of tumor resectability is critical to determining the most adequate therapy for gastric cancer. The aim of this study is to identify a possible link between 18F-fluorodeoxyglucose (18F-FDG) uptake on PET scan combined with CT scan (PET/CT) and predictions of lymph node metastasis and non-curative surgery.
METHODS
This study included 156 gastric cancer patients who underwent preoperative 18F-FDG PET/CT and surgery. In cases with perceptible FDG uptake in the primary tumor or lymph nodes, the maximum standardized uptake value (SUVmax) was calculated.
RESULTS
In multivariate analysis, non-curative surgery (OR, 11.05; 95% CI, 1.10-111.08; p=0.041), tumor size (> or =3 cm) (OR, 7.39; 95% CI, 2.41-22.70; p<0.001), and lymph node metastasis (OR, 5.47; 95% CI, 2.05-14.64; p=0.001) were significant independent predictors for 18F-FDG uptake in the primary tumors. Tumor size (tumor size > or =3 cm) (OR, 3.15; 95% CI, 1.16-8.58; p=0.025) and lymph node metastasis (OR, 3.36; 95% CI, 1.23-9.14; p=0.018) showed significant association with 18F-FDG uptake in lymph node. When the SUVmax of the primary gastric tumor was greater than 3.75, the sensitivity and specificity of PET/CT with regard to the diagnosis of metastatic lymph node were 73.5% and 74.5%. When the SUVmax of the primary gastric tumor was greater than 4.35 and the FDG uptake of lymph nodes was positive, non-curative surgery was predicted with a sensitivity of 58.8% and specificity of 91.6%.
CONCLUSIONS
A high FDG uptake of the gastric tumor was related to histologic positive lymph nodes and non-curative surgery.
MeSH Terms
-
Adult
Aged
Aged, 80 and over
Area Under Curve
Carcinoma/*diagnosis/pathology/surgery
Female
Fluorodeoxyglucose F18
Humans
Lymph Nodes/surgery
Lymphatic Metastasis/radionuclide imaging
Male
Middle Aged
Neoplasm Staging
Odds Ratio
Peritoneal Neoplasms/diagnosis/secondary
Positron-Emission Tomography
ROC Curve
Regression Analysis
Stomach Neoplasms/*diagnosis/pathology/surgery
Tomography, X-Ray Computed
Fluorodeoxyglucose F18
Figure
-
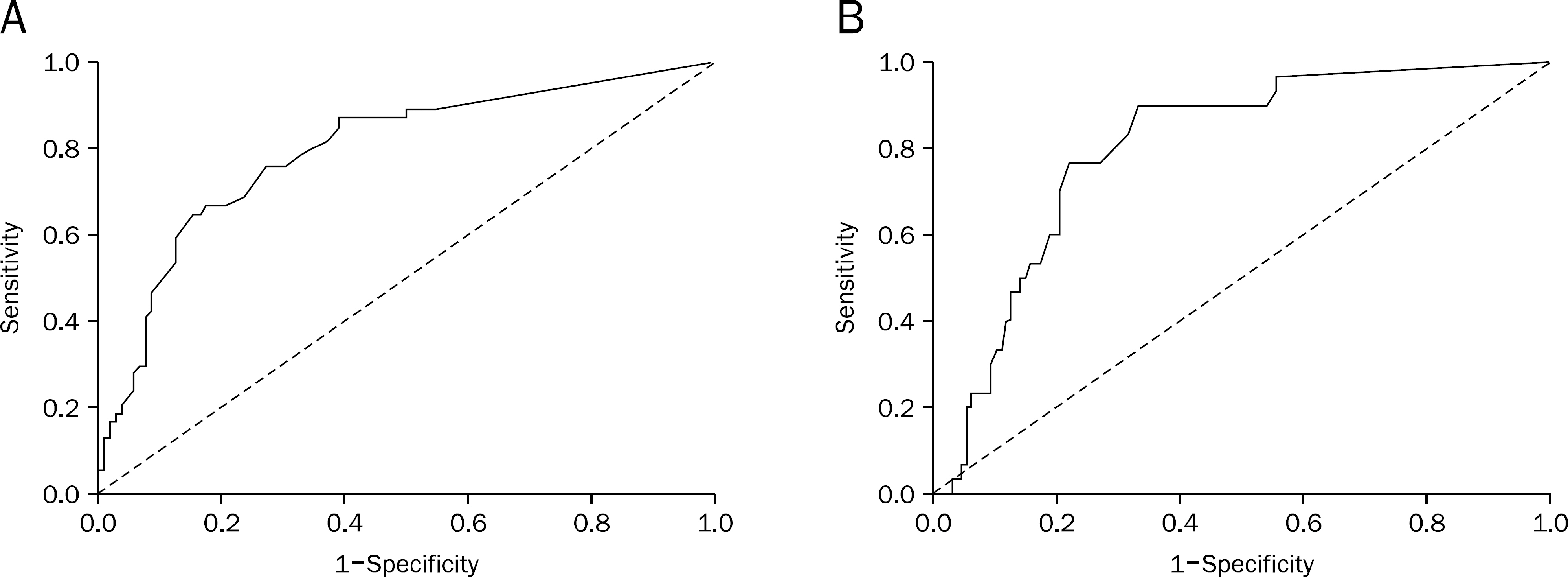
Fig. 1. Receiver operator characteristics (ROC) curve of the maximum standardized uptake value (SUVmax) of primary tumor. (A) In ROC for detecting lymph node metastasis, an area under the curve of 0.795 was obtained (95% CI, 0.719-0.871; p<0.001). (B) In ROC for predicting non-curative surgery, area under the curve was 0.801 (95% CI, 0.722-0.879; p<0.001).
Reference
-
References
1. Kim SK, Kang KW, Lee JS, et al. Assessment of lymph node metastases using 18F-FDG PET in patients with advanced gastric cancer. Eur J Nucl Med Mol Imaging. 2006; 33:148–155.
Article2. Yeung HW, Macapinlac H, Karpeh M, Finn RD, Larson SM. Accuracy of FDG-PET in gastric cancer. Preliminary experience. Clin Positron Imaging. 1998; 1:213–221.
Article3. Stahl A, Ott K, Weber WA, et al. FDG PET imaging of locally advanced gastric carcinomas: correlation with endoscopic and histopathological findings. Eur J Nucl Med Mol Imaging. 2003; 30:288–295.
Article4. Mochiki E, Kuwano H, Katoh H, Asao T, Oriuchi N, Endo K. Evaluation of 18F-2-deoxy-2-fluoro-D-glucose positron emission tomography for gastric cancer. World J Surg. 2004; 28:247–253.
Article5. Chen J, Cheong JH, Yun MJ, et al. Improvement in preoperative staging of gastric adenocarcinoma with positron emission tomography. Cancer. 2005; 103:2383–2390.
Article6. Yun M, Lim JS, Noh SH, et al. Lymph node staging of gastric cancer using (18)F-FDG PET: a comparison study with CT. J Nucl Med. 2005; 46:1582–1588.7. Ajani J, Bekaii-Saab T, D'Amico TA, et al. Gastric cancer clinical practice guidelines. J Natl Compr Canc Netw. 2006; 4:350–366.
Article8. Hur H, Kim SH, Kim W, Song KY, Park CH, Jeon HM. The efficacy of preoperative PET/CT for prediction of curability in surgery for locally advanced gastric carcinoma. World J Surg Oncol. 2010; 8:86.
Article9. Bentrem D, Gerdes H, Tang L, Brennan M, Coit D. Clinical correlation of endoscopic ultrasonography with pathologic stage and outcome in patients undergoing curative resection for gastric cancer. Ann Surg Oncol. 2007; 14:1853–1859.
Article10. Burke EC, Karpeh MS, Conlon KC, Brennan MF. Laparoscopy in the management of gastric adenocarcinoma. Ann Surg. 1997; 225:262–267.
Article11. Dassen AE, Lips DJ, Hoekstra CJ, Pruijt JF, Bosscha K. FDG-PET has no definite role in preoperative imaging in gastric cancer. Eur J Surg Oncol. 2009; 35:449–455.
Article12. Bombardieri E, Aktolun C, Baum RP, et al. FDG-PET: procedure guidelines for tumour imaging. Eur J Nucl Med Mol Imaging. 2003; 30:BP115–BP124.
Article13. Mukai K, Ishida Y, Okajima K, Isozaki H, Morimoto T, Nishiyama S. Usefulness of preoperative FDG-PET for detection of gastric cancer. Gastric Cancer. 2006; 9:192–196.
Article14. Akagi T, Shiraishi N, Kitano S. Lymph node metastasis of gastric cancer. Cancers (Basel). 2011; 3:2141–2159.
Article15. Duhaylongsod FG, Lowe VJ, Patz EF Jr, Vaughn AL, Coleman RE, Wolfe WG. Lung tumor growth correlates with glucose metabo-lism measured by fluoride-18 fluorodeoxyglucose positron emission tomography. Ann Thorac Surg. 1995; 60:1348–1352.
Article16. Adler LP, Blair HF, Williams RP, et al. Grading liposarcomas with PET using [18F]FDG. J Comput Assist Tomogr. 1990; 14:960–962.
Article17. Yoshioka T, Yamaguchi K, Kubota K, et al. Evaluation of 18F-FDG PET in patients with advanced, metastatic, or recurrent gastric cancer. J Nucl Med. 2003; 44:690–699.18. Shreve PD, Anzai Y, Wahl RL. Pitfalls in oncologic diagnosis with FDG PET imaging: physiologic and benign variants. Radiograph-ics. 1999; 19:61–77.
Article19. Cook GJ, Maisey MN, Fogelman I. Normal variants, artefacts and interpretative pitfalls in PET imaging with 18-fluoro-2-deoxy-glucose and carbon-11 methionine. Eur J Nucl Med. 1999; 26:1363–1378.
Article20. Ames J, Blodgett T, Meltzer C. 18F-FDG uptake in an ovary containing a hemorrhagic corpus luteal cyst: false-positive PET/CT in a patient with cervical carcinoma. AJR Am J Roentgenol. 2005; 185:1057–1059.
Article21. Lerman H, Metser U, Grisaru D, Fishman A, Lievshitz G, Even-Sapir E. Normal and abnormal 18F-FDG endometrial and ovarian uptake in pre- and postmenopausal patients: assessment by PET/CT. J Nucl Med. 2004; 45:266–271.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- 18F-2-Deoxy-2-Fluoro-D-Glucose Positron Emission Tomography: Computed Tomography for Preoperative Staging in Gastric Cancer Patients
- Prediction of Axillary Nodal Status according to the Axillary Lymph Node to Primary Breast Tumor Maximum Standardized Uptake Value Ratio on 18F-fluorodeoxyglucose Positron Emission Tomography/Computed Tomography
- F18-fluorodeoxyglucose-positron emission tomography and computed tomography is not accurate in preoperative staging of gastric cancer
- Supraclavicular Lymph Node Metastasis from Various Malignancies: Assessment with 18F-Fluorodeoxyglucose Positron Emission Tomography/CT, Contrast-Enhanced CT and Ultrasound
- Reliability of 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography in the Nodal Staging of Colorectal Cancer Patients
