J Korean Med Sci.
2015 Jun;30(6):710-715. 10.3346/jkms.2015.30.6.710.
Stereotactic Body Radiation Therapy for Low- to Intermediate-risk Prostate Adenocarcinoma
- Affiliations
-
- 1Department of Radiation Oncology, Gyeongsang National University School of Medicine, Jinju, Korea. jsk92@gnu.ac.kr
- 2Department of Urology, Gyeongsang National University School of Medicine, Jinju, Korea.
- 3Institute of Health Science, Gyeongsang National University, Jinju, Korea.
- KMID: 2160598
- DOI: http://doi.org/10.3346/jkms.2015.30.6.710
Abstract
- The aim of the present study was to evaluate the efficacy and toxicity of stereotactic body radiation therapy (SBRT) for low- to intermediate-risk prostate adenocarcinoma. Thirty-nine patients were retrospectively reviewed. The SBRT was delivered using the CyberKnife with the fiducial tracking method combined with In-tempo imaging. The gross target volume, which included the prostate only, was delineated on the fused CT/MRI scans. The prescription dose was delivered every other day as 5 fractions of 7.5 Gy. Venous blood was obtained before and after SBRT to assess the prostate-specific antigen (PSA) level. Toxicity was evaluated using the CTCAE, v4.03. The median follow-up time was 30.0 months. The median initial PSA level was 7.7 ng/mL. PSA levels decreased in all patients treated with SBRT, and after 5 months, the median PSA was less than 2 ng/mL. The rate of overall 3-yr actuarial biochemical failure free survival was 93.9%. Acute side effects were generally comparable with those of previous studies. The PSA change and toxicity after SBRT for low- to intermediate-risk prostate adenocarcinoma indicates favorable biochemical responses and tolerable levels of toxicity. Additionally short course treatment may produce cost benefit and convenience to patients.
Keyword
MeSH Terms
Figure
-
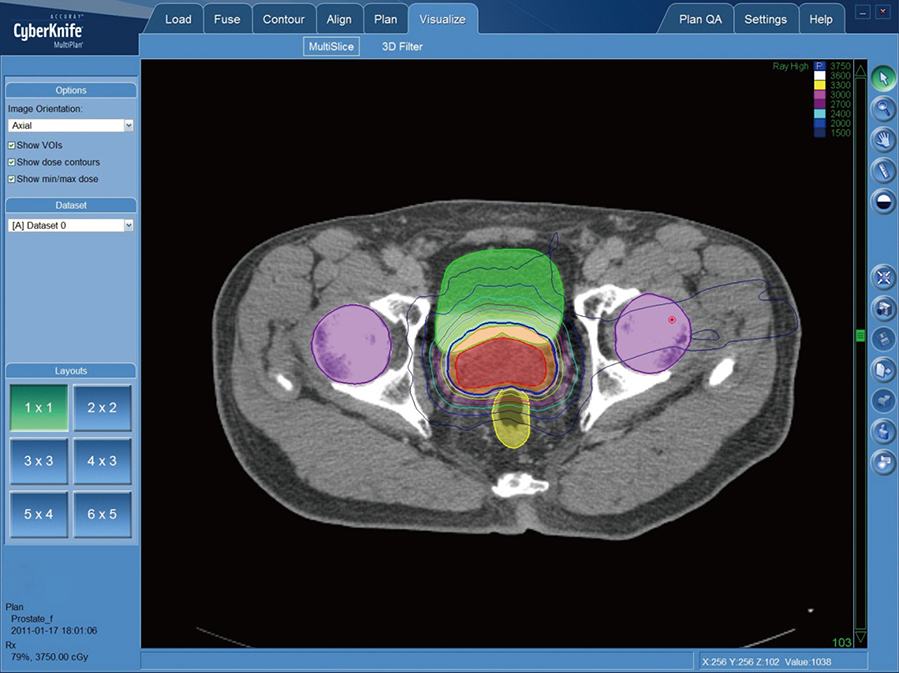
Fig. 1 Example of CyberKnife SBRT treatment plan showing an axial view in a 70-yr old man who was diagnosed with adenocarcinoma of the prostate (cT1c; initial PSA: 3.01; GS: 7).
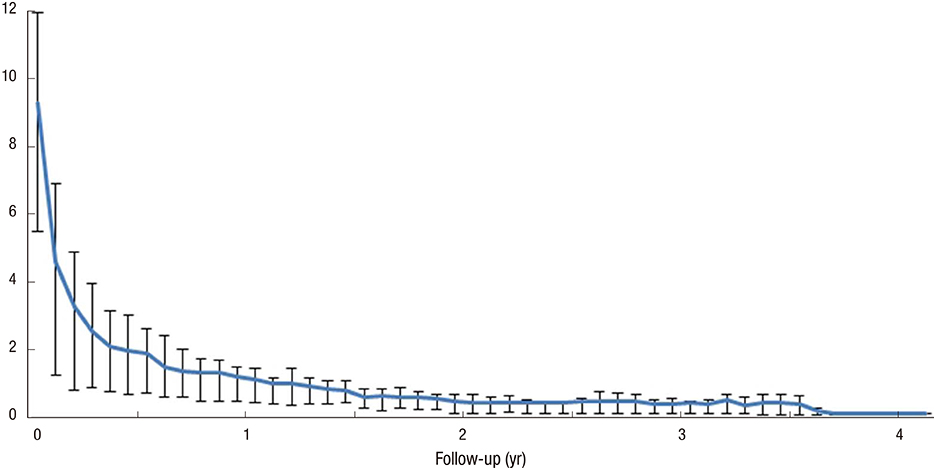
Fig. 2 Change of median PSA value with IQR after SBRT (25%-75%).
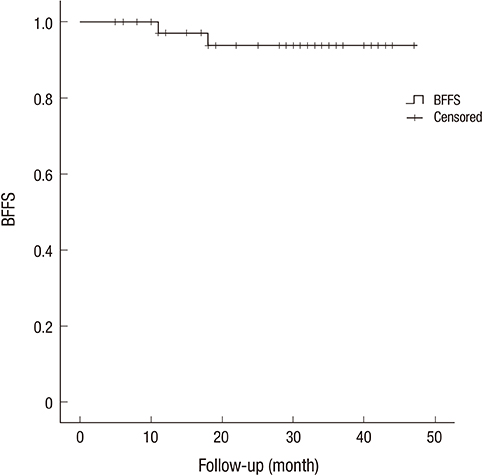
Fig. 3 BFFS for the low- to intermediate-risk group patients with prostate adenocarcinoma.
Cited by 1 articles
-
Analysis of Motion-dependent Clinical Outcome of Tumor Tracking Stereotactic Body Radiotherapy for Prostate Cancer
Hoon Sik Choi, Ki Mun Kang, Bae Kwon Jeong, Jin Ho Song, Yun Hee Lee, In Bong Ha, Sung Chul Kam, Jeong Seok Hwa, Jae Seog Hyun, Jungmo Do, Dong Hyeok Jeong, Hojin Jeong
J Korean Med Sci. 2018;33(14):. doi: 10.3346/jkms.2018.33.e107.
Reference
-
1. Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011; 61:69–90.2. Thompson I, Thrasher JB, Aus G, Burnett AL, Canby-Hagino ED, Cookson MS, D'Amico AV, Dmochowski RR, Eton DT, Forman JD, et al. AUA Prostate Cancer Clinical Guideline Update Panel. Guideline for the management of clinically localized prostate cancer: 2007 update. J Urol. 2007; 177:2106–2131.3. Brenner DJ, Hall EJ. Fractionation and protraction for radiotherapy of prostate carcinoma. Int J Radiat Oncol Biol Phys. 1999; 43:1095–1101.4. D'Souza WD, Thames HD. Is the alpha/beta ratio for prostate cancer low? Int J Radiat Oncol Biol Phys. 2001; 51:1–3.5. King CR, Fowler JF. A simple analytic derivation suggests that prostate cancer alpha/beta ratio is low. Int J Radiat Oncol Biol Phys. 2001; 51:213–214.6. Miralbell R, Roberts SA, Zubizarreta E, Hendry JH. Dose-fractionation sensitivity of prostate cancer deduced from radiotherapy outcomes of 5,969 patients in seven international institutional datasets: alpha/beta = 1.4 (0.9-2.2) Gy. Int J Radiat Oncol Biol Phys. 2012; 82:e17–e24.7. Lukka H, Hayter C, Julian JA, Warde P, Morris WJ, Gospodarowicz M, Levine M, Sathya J, Choo R, Prichard H, et al. Randomized trial comparing two fractionation schedules for patients with localized prostate cancer. J Clin Oncol. 2005; 23:6132–6138.8. Yeoh EE, Botten RJ, Butters J, Di Matteo AC, Holloway RH, Fowler J. Hypofractionated versus conventionally fractionated radiotherapy for prostate carcinoma: final results of phase III randomized trial. Int J Radiat Oncol Biol Phys. 2011; 81:1271–1278.9. Madsen BL, Hsi RA, Pham HT, Fowler JF, Esagui L, Corman J. Stereotactic hypofractionated accurate radiotherapy of the prostate (SHARP), 33.5 Gy in five fractions for localized disease: first clinical trial results. Int J Radiat Oncol Biol Phys. 2007; 67:1099–1105.10. King CR, Lehmann J, Adler JR, Hai J. CyberKnife radiotherapy for localized prostate cancer: rationale and technical feasibility. Technol Cancer Res Treat. 2003; 2:25–30.11. Aluwini S, van Rooij P, Hoogeman M, Bangma C, Kirkels WJ, Incrocci L, Kolkman-Deurloo IK. CyberKnife stereotactic radiotherapy as monotherapy for low- to intermediate-stage prostate cancer: early experience, feasibility, and tolerance. J Endourol. 2010; 24:865–869.12. King CR, Brooks JD, Gill H, Presti JC Jr. Long-term outcomes from a prospective trial of stereotactic body radiotherapy for low-risk prostate cancer. Int J Radiat Oncol Biol Phys. 2012; 82:877–882.13. Freeman DE, King CR. Stereotactic body radiotherapy for low-risk prostate cancer: five-year outcomes. Radiat Oncol. 2011; 6:3.14. Michalski JM, Moughan J, Purdy JA, Bosch WR, Bahary J, Lau H, Duclos M, Parliament M, Morton G, Hamstra DA, et al. Initial Results of a Phase 3 Randomized Study of High Dose 3DCRT/IMRT versus Standard Dose 3D-CRT/IMRT in Patients Treated for Localized Prostate Cancer (RTOG 0126). Int J Radiat Oncol Biol Phys. 2014; 90:1263.15. Abramowitz MC, Li T, Buyyounouski MK, Ross E, Uzzo RG, Pollack A, Horwitz EM. The Phoenix definition of biochemical failure predicts for overall survival in patients with prostate cancer. Cancer. 2008; 112:55–60.16. Stock RG, Stone NN, Cesaretti JA. Prostate-specific antigen bounce after prostate seed implantation for localized prostate cancer: descriptions and implications. Int J Radiat Oncol Biol Phys. 2003; 56:448–453.17. Nakamura K, Akimoto T, Mizowaki T, Hatano K, Kodaira T, Nakamura N, Kozuka T, Shikama N, Kagami Y. Patterns of practice in intensity-modulated radiation therapy and image-guided radiation therapy for prostate cancer in Japan. Jpn J Clin Oncol. 2012; 42:53–57.18. Namiki S, Ishidoya S, Ito A, Tochigi T, Numata I, Narazaki K, Yamada S, Takai Y, Arai Y. Five-year follow-up of health-related quality of life after intensity-modulated radiation therapy for prostate cancer. Jpn J Clin Oncol. 2009; 39:732–738.19. McBride SM, Wong DS, Dombrowski JJ, Harkins B, Tapella P, Hanscom HN, Collins SP, Kaplan ID. Hypofractionated stereotactic body radiotherapy in low-risk prostate adenocarcinoma: preliminary results of a multi-institutional phase 1 feasibility trial. Cancer. 2012; 118:3681–3690.20. King CR, Brooks JD, Gill H, Pawlicki T, Cotrutz C, Presti JC Jr. Stereotactic body radiotherapy for localized prostate cancer: interim results of a prospective phase II clinical trial. Int J Radiat Oncol Biol Phys. 2009; 73:1043–1048.21. Boike TP, Lotan Y, Cho LC, Brindle J, DeRose P, Xie XJ, Yan J, Foster R, Pistenmaa D, Perkins A, et al. Phase I dose-escalation study of stereotactic body radiation therapy for low- and intermediate-risk prostate cancer. J Clin Oncol. 2011; 29:2020–2026.22. Hinnen KA, Monninkhof EM, Battermann JJ, van Roermund JG, Frank SJ, van Vulpen M. Prostate specific antigen bounce is related to overall survival in prostate brachytherapy. Int J Radiat Oncol Biol Phys. 2012; 82:883–888.23. Yu JB, Cramer LD, Herrin J, Soulos PR, Potosky AL, Gross CP. Stereotactic body radiation therapy versus intensity-modulated radiation therapy for prostate cancer: comparison of toxicity. J Clin Oncol. 2014; 32:1195–1201.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hypofractionated stereotactic body radiotherapy in low- and intermediate-risk prostate carcinoma
- Stereotactic Body Radiation Therapy
- Change of serum prostate specific antigen values after radiation therapy in prostate cancer
- Stereotactic radiotherapy of the prostate: fractionation and utilization in the United States
- Low-Dose-Rate Brachytherapy for Low- and Intermediate-Risk Groups of Localized Prostate Cancer
