Yonsei Med J.
2013 Jul;54(4):965-972. 10.3349/ymj.2013.54.4.965.
Acute Kidney Injury in Patients with Sepsis and Septic Shock: Risk Factors and Clinical Outcomes
- Affiliations
-
- 1Department of Internal Medicine, Chonnam National University Medical School, Gwangju, Korea. skimw@chonnam.ac.kr
- KMID: 2158233
- DOI: http://doi.org/10.3349/ymj.2013.54.4.965
Abstract
- PURPOSE
The aim of this study was to investigate clinical characteristics and risk factors of acute kidney injury (AKI) in patients with sepsis and septic shock. Additionally, we explored whether the severity of AKI affects on the clinical outcomes.
MATERIALS AND METHODS
Data were collected retrospectively in a single center. Among 5680 patients who visited emergency department from January to December 2010, 992 patients with sepsis and septic shock were enrolled. Patients were divided into two groups, patients who developed AKI or not, to compare the baseline characteristics, and laboratory and physiologic data. Patients with AKI were subdivided according to its stages for survival analysis.
RESULTS
AKI was developed in 57.7% of patients. Multivariable logistic regression analysis revealed that development of septic AKI was associated with older age, pre-existing chronic kidney disease, use of angiotensin converting enzyme inhibitor or angiotensin receptor blocker, presence of shock, positive blood culture results, and low white blood cell and platelet counts. Hospital mortality was higher in AKI group. Crude Kaplan-Meier survival curves demonstrated reduced 30-day survival rate was significantly associated with the severity of acute kidney injury.
CONCLUSION
The development of septic AKI was associated with poor clinical outcomes. Furthermore, the severity of AKI was associated with increased mortality.
Keyword
MeSH Terms
-
Acute Kidney Injury/*etiology/mortality
Age Factors
Aged
Angiotensin-Converting Enzyme Inhibitors/therapeutic use
Female
Humans
Kaplan-Meier Estimate
Logistic Models
Male
Middle Aged
Renal Insufficiency, Chronic/complications
Retrospective Studies
Risk Factors
Sepsis/*complications/*mortality
Shock, Septic/*complications/*mortality
Survival Rate
Angiotensin-Converting Enzyme Inhibitors
Figure
-
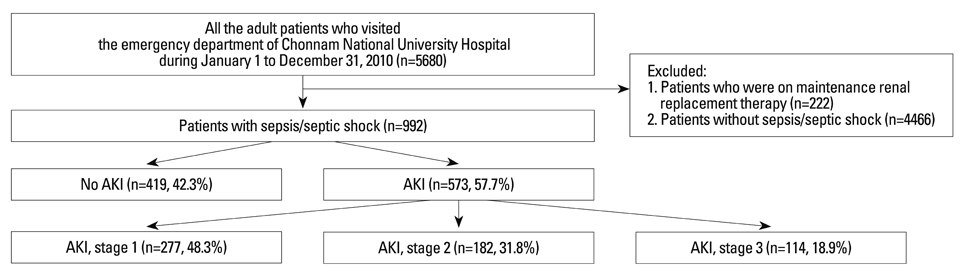
Fig. 1 Study design. AKI, acute kidney injury.

Fig. 2 Survival curves for 30 days. Kaplan-Meier survival for 30 days by AKI stages in patients with sepsis and septic shock demonstrated reduced survival rate was significantly associated with the severity of AKI (p<0.001 by log-rank test). AKI, acute kidney injury.
Reference
-
1. Cartin-Ceba R, Haugen EN, Iscimen R, Trillo-Alvarez C, Juncos L, Gajic O. Evaluation of "Loss" and "End stage renal disease" after acute kidney injury defined by the Risk, Injury, Failure, Loss and ESRD classification in critically ill patients. Intensive Care Med. 2009; 35:2087–2095.
Article2. Hoste EA, Schurgers M. Epidemiology of acute kidney injury: how big is the problem? Crit Care Med. 2008; 36:4 Suppl. S146–S151.
Article3. Bagshaw SM, Uchino S, Bellomo R, Morimatsu H, Morgera S, Schetz M, et al. Septic acute kidney injury in critically ill patients: clinical characteristics and outcomes. Clin J Am Soc Nephrol. 2007; 2:431–439.
Article4. Plataki M, Kashani K, Cabello-Garza J, Maldonado F, Kashyap R, Kor DJ, et al. Predictors of acute kidney injury in septic shock patients: an observational cohort study. Clin J Am Soc Nephrol. 2011; 6:1744–1751.
Article5. Bagshaw SM, Lapinsky S, Dial S, Arabi Y, Dodek P, Wood G, et al. Acute kidney injury in septic shock: clinical outcomes and impact of duration of hypotension prior to initiation of antimicrobial therapy. Intensive Care Med. 2009; 35:871–881.
Article6. Oppert M, Engel C, Brunkhorst FM, Bogatsch H, Reinhart K, Frei U, et al. Acute renal failure in patients with severe sepsis and septic shock--a significant independent risk factor for mortality: results from the German Prevalence Study. Nephrol Dial Transplant. 2008; 23:904–909.
Article7. Langenberg C, Wan L, Egi M, May CN, Bellomo R. Renal blood flow in experimental septic acute renal failure. Kidney Int. 2006; 69:1996–2002.
Article8. Langenberg C, Wan L, Bagshaw SM, Egi M, May CN, Bellomo R. Urinary biochemistry in experimental septic acute renal failure. Nephrol Dial Transplant. 2006; 21:3389–3397.
Article9. Brenner M, Schaer GL, Mallory DL, Suffredini AF, Parrillo JE. Detection of renal blood flow abnormalities in septic and critically ill patients using a newly designed indwelling thermodilution renal vein catheter. Chest. 1990; 98:170–179.
Article10. Langenberg C, Wan L, Egi M, May CN, Bellomo R. Renal blood flow and function during recovery from experimental septic acute kidney injury. Intensive Care Med. 2007; 33:1614–1618.
Article11. Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P. Acute Dialysis Quality Initiative workgroup. Acute renal failure - definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2004; 8:R204–R212.12. Neveu H, Kleinknecht D, Brivet F, Loirat P, Landais P. The French Study Group on Acute Renal Failure. Prognostic factors in acute renal failure due to sepsis Results of a prospective multicentre study. Nephrol Dial Transplant. 1996; 11:293–299.
Article13. Levey AS, Coresh J, Greene T, Stevens LA, Zhang YL, Hendriksen S, et al. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann Intern Med. 2006; 145:247–254.
Article14. Knaus W, Wagner D, Draper E. APACHE III study design: analytic plan for evaluation of severity and outcome in intensive care unit patients. Development of APACHE. Crit Care Med. 1989; 17(12 Pt 2):S181–S185.15. Bone RC, Sibbald WJ, Sprung CL. The ACCP-SCCM consensus conference on sepsis and organ failure. Chest. 1992; 101:1481–1483.
Article16. Bagshaw SM, George C, Bellomo R. ANZICS Database Management Committee. Early acute kidney injury and sepsis: a multicentre evaluation. Crit Care. 2008; 12:R47.
Article17. Kumar A, Roberts D, Wood KE, Light B, Parrillo JE, Sharma S, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006; 34:1589–1596.
Article18. Bentley ML, Corwin HL, Dasta J. Drug-induced acute kidney injury in the critically ill adult: recognition and prevention strategies. Crit Care Med. 2010; 38:6 Suppl. S169–S174.
Article19. Pannu N, Nadim MK. An overview of drug-induced acute kidney injury. Crit Care Med. 2008; 36:4 Suppl. S216–S223.
Article20. Tracey KJ, Beutler B, Lowry SF, Merryweather J, Wolpe S, Milsark IW, et al. Shock and tissue injury induced by recombinant human cachectin. Science. 1986; 234:470–474.
Article21. Okusawa S, Gelfand JA, Ikejima T, Connolly RJ, Dinarello CA. Interleukin 1 induces a shock-like state in rabbits. Synergism with tumor necrosis factor and the effect of cyclooxygenase inhibition. J Clin Invest. 1988; 81:1162–1172.
Article22. Nechemia-Arbely Y, Barkan D, Pizov G, Shriki A, Rose-John S, Galun E, et al. IL-6/IL-6R axis plays a critical role in acute kidney injury. J Am Soc Nephrol. 2008; 19:1106–1115.
Article23. Yu DH, Kim B, Park J. Pathophysiologic and immunologic changes in a canine endotoxemia over a period of 24 hours. J Vet Med Sci. 2012; 74:537–544.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment Guidelines of Sepsis and Septic Shock
- Clinical Characteristics and Outcomes of Septic Acute Kidney Injury in Critically Ill Patients
- Recent Evidences of Sepsis Treatment
- Current Insights into Sepsis Treatments
- Is Intravenous Contrast-Enhanced Computed Tomography Dangerous in Patients with Elevated Serum Creatinine?
