Diagnosis of Pseudoangiomatous Stromal Hyperplasia of the Breast: Ultrasonography Findings and Different Biopsy Methods
- Affiliations
-
- 1Department of Radiology, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea. claudel@skku.edu
- 2Department of Radiology, Center for Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2158194
- DOI: http://doi.org/10.3349/ymj.2008.49.5.757
Abstract
- PURPOSE
Pseudoangiomatous stromal hyperplasia (PASH) of the breast is a rare, benign condition that can be mistaken as a fibroadenoma on an ultrasound examination or as a low-grade angiosarcoma on a histological examination. The objective of this study was to evaluate the ultrasound features and to present biopsy methods to correctly identify PASH. PATIENTS AND METHODS: We retrospectively reviewed the data of 55 women who were diagnosed with PASH of the breast. Ultrasound features were evaluated according to the Breast Imaging Reporting and Data System (BI-RADS; American College of Radiology). The diagnostic ability of different biopsy methods such as core needle biopsy, vacuum-assisted biopsy and excisional biopsy were analyzed with the final histopathological results of surgical specimens. RESULTS: PASH presented as a circumscribed solid mass, with hypoechoic texture with or without heterogeneity, and a parallel orientation. The features of small, internal cysts or vascular channels and no calcifications can be used to differentiate the lesions from fibroadenomas. A core needle biopsy misdiagnosed PASH in 13 cases out of 28 cases and vacuum-assisted biopsy correctly identified PASH in all 3 cases. CONCLUSION: Ultrasound features of PASH should be noted when performing a biopsy. For inconclusive cases of PASH, an excisional biopsy followed by an initial core biopsy should be performed.
MeSH Terms
Figure
-

Fig. 1 Transverse sonography of PASH shows an approximate 5 cm sized well-circumscribed homogeneous hypoechoic oval mass in a 30-year-old woman who presented with a palpable mass in the right breast. PASH, pseudoangiomatous stromal hyperplasia.
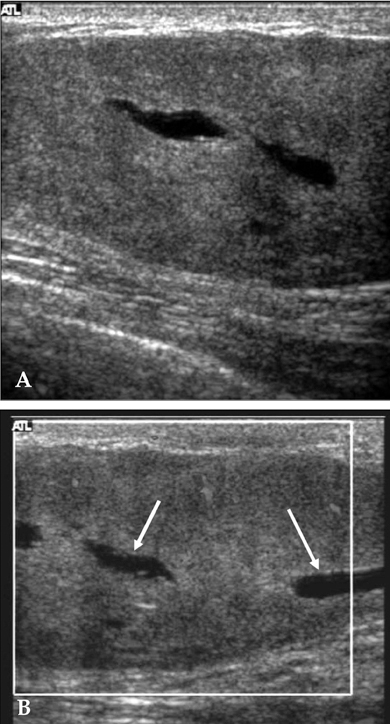
Fig. 2 (A) Sonography demonstrates a well-circumscribed homogeneous hypoechoic mass. (B) Doppler US shows vascular channels (arrows) in the lesion. In these cases, a histological examination also identified the presence of vascular channels. US, ultrasound.
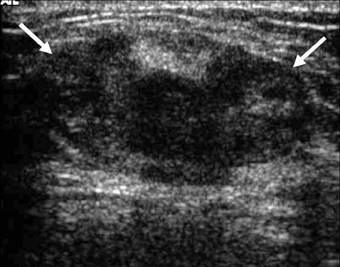
Fig. 3 Fibrocystic change was confirmed after an initial core needle biopsy, but surgical excision identified PASH in a 42-year-old premenopausal woman with BI-RADS category 4a. US shows a 2.8 cm sized heterogeneous echoic nodule mixed with an ill-defined margin with an irregular shape. PASH, pseudoangiomatous stromal hyperplasia; BI-RADS, breast imaging reporting and data system; US, ultrasound.
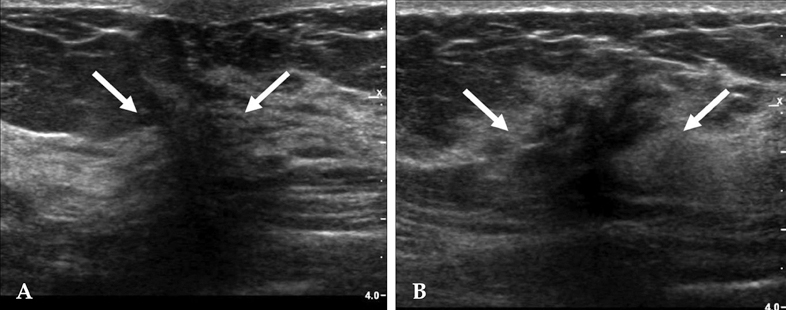
Fig. 4 Transverse (A) and longitudinal (B) breast US scans. A nodule, characterized as BI-RADS category 4b, was irregular in shape, not parallel to the breast axis with a spiculated margin, and was hypoechoic with posterior shadowing and an echogenic halo, which presented as a cancer or radial scar. This case was originally diagnosed after a core biopsy and was confirmed as stromal fibrosis, but an excisional biopsy identified the lesion as PASH. BI-RADS, breast imaging reporting and data system; PASH, pseudoangiomatous stromal hyperplasia; US, ultrasound.

Fig. 5 Transverse (A) and longitudinal (B) breast US scans. This circumscribed round but not parallel to the chest wall PASH lesion was initially diagnosed as a fibroadenoma after a core biopsy. PASH, pseudoangiomatous stromal hyperplasia; US, ultrasound.
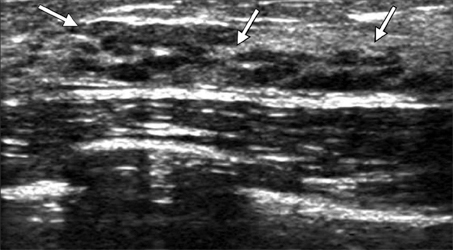
Fig. 6 Non-mass-forming PASH. PASH was depicted not as a mass but as low echoic lesions intermingled with the normal parenchyma. The initial pathological diagnosis of this case was fibrocystic change, but the lesion was identified as PASH after surgical excision. PASH, pseudoangiomatous stromal hyperplasia.
Reference
-
1. Vuitch MF, Rosen PP, Erlandson RA. Pseudoangiomatous hyperplasia of mammary stroma. Hum Pathol. 1986. 17:185–191.
Article2. Cohen MA, Morris EA, Rosen PP, Dershaw DD, Liberman L, Abramson AF. Pseudoangiomatous stromal hyperplasia: mammographic, sonographic, and clinical patterns. Radiology. 1996. 198:117–120.
Article3. Goel NB, Knight TE, Pandey S, Riddick-Young M, de Paredes ES, Trivedi A. Fibrous lesions of the breast: imaging-pathologic correlation. Radiographics. 2005. 25:1547–1559.
Article4. Mercado CL, Naidrich SA, Hamele-Bena D, Fineberg SA, Buchbinder SS. Pseudoangiomatous stromal hyperplasia of the breast: sonographic features with histopathologic correlation. Breast J. 2004. 10:427–432.
Article5. Mendelson EB, Baum JK, Berg WA, Merritt CR, Rubin E. . Ultrasound. Breast Imaging Reporting and Data System (BI-RADS). 2003. 4th ed. Reston, Va: American College of Radiology.6. Powell CM, Cranor ML, Rosen PP. Pseudoangiomatous stromal hyperplasia (PASH). A mammary stromal tumor with myofibroblastic differentiation. Am J Surg Pathol. 1995. 19:270–277.7. Brogi E. Benign and malignant spindle cell lesions of the breast. Semin Diagn Pathol. 2004. 21:57–64.
Article8. Piccoli CW, Feig SA, Palazzo JP. Developing asymmetric breast tissue. Radiology. 1999. 211:111–117.
Article9. Rosen PP. Rosen PP, editor. Benign mesenchymal neoplasms. Rosen's breast pathology. 1997. Philidelphia, PA: Lippincott Raven.10. Polger MR, Denison CM, Lester S, Meyer JE. Pseudoangiomatous stromal hyperplasia: mammographic and sonographic appearances. AJR Am J Roentgenol. 1996. 166:349–352.
Article11. Aron M, Ray R, Verma K. Pseudoangiomatous stromal hyperplasia of the breast-cytological features of two cases and review of literature. Indian J Pathol Microbiol. 2005. 48:260–264.12. Levine PH, Nimeh D, Guth AA, Cangiarella JF. Aspiration biopsy of nodular pseudoangiomatous stromal hyperplasia of the breast: clinicopathologic correlates in 10 cases. Diagn Cytopathol. 2005. 32:345–350.
Article13. Lui PC, Law BK, Chu WC, Pang LM, Tse GM. Fine-needle aspiration cytology of pseudoangiomatous stromal hyperplasia of the breast. Diagn Cytopathol. 2004. 30:353–355.
Article14. Spitz DJ, Reddy VB, Gattuso P. Fine-needle aspiration of pseudoangiomatous stromal hyperplasia of the breast. Diagn Cytopathol. 1999. 20:323–324.
Article15. Hoda SA, Rosen PP. Observations on the pathologic diagnosis of selected unusual lesions in needle core biopsies of breast. Breast J. 2004. 10:522–527.
Article16. Tagaya N, Nakagawa A, Ishikawa Y, Oyama T, Kubota K. Experience with ultrasonographically guided vacuum-assisted resection of benign breast tumors. Clin Radiol. 2008. 63:396–400.
Article17. Ibrahim RE, Sciotto CG, Weidner N. Pseudoangiomatous hyperplasia of mammary stroma. Some observations regarding its clinicopathologic spectrum. Cancer. 1989. 63:1154–1160.
Article18. Sng KK, Tan SM, Mancer JF, Tay KH. The contrasting presentation and management of pseudoangiomatous stromal hyperplasia of the breast. Singapore Med J. 2008. 49:e82–e85.19. Pruthi S, Reynolds C, Johnson RE, Gisvold JJ. Tamoxifen in the management of pseudoangiomatous stromal hyperplasia. Breast J. 2001. 7:434–439.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pseudoangiomatous Stromal Hyperplasia of the Breast Appearing as a Giant Mass: A Case Report
- Mass Forming Pseudoangiomatous Stromal Hyperplasia of the Breast: Sonographic Features
- Rapidly Growing Bilateral Pseudoangiomatous Stromal Hyperplasia of the Breast
- Radiologic Imaging Findings of Bilateral Infiltrating Pseudoangiomatous Stromal Hyperplasia of the Breasts: A Case Report
- Huge Bilateral Breast Hamartoma Accompanied with Pseudoangiomatous Stromal Hyperplasia
