Barotrauma after Manual Ventilation in a Patient with Life-Threatening Massive Hemoptysis
- Affiliations
-
- 1Division of Pulmonary Medicine, Department of Internal Medicine, Seoul St. Mary's Hospital, The Catholic University of Korea, Seoul, Korea. chinkook@catholic.ac.kr
- 2Department of Internal Medicine, The Catholic University of Korea, Seoul, Korea.
- KMID: 2156186
- DOI: http://doi.org/10.4266/kjccm.2015.30.4.308
Abstract
- A 36-year-old female patient with aplastic anemia developed massive hemoptysis and was placed on ventilator support. However, airway obstruction by blood clots triggered desaturation and ventilator malfunction. Manual ventilation was initiated to improve oxy-genation, and emergency flexible bronchoscopy was performed to clear the airway. Nevertheless, the patient developed extensive subcutaneous emphysema, pneumothorax, and pneumomediastinum.
Keyword
MeSH Terms
Figure
-
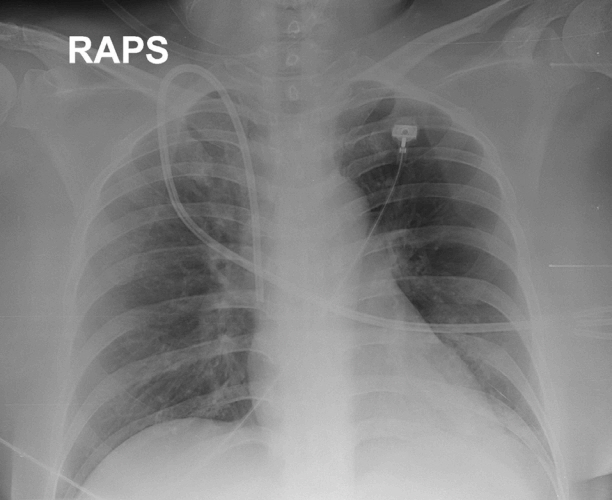
Fig. 1. A chest radiograph reveals a short, thick, subsegmental atelectasis in the lingular division of the left lung. A Hickman catheter was inserted into the superior vena cava via the right internal jugular vein. RAPS: right anterior posterior supine.
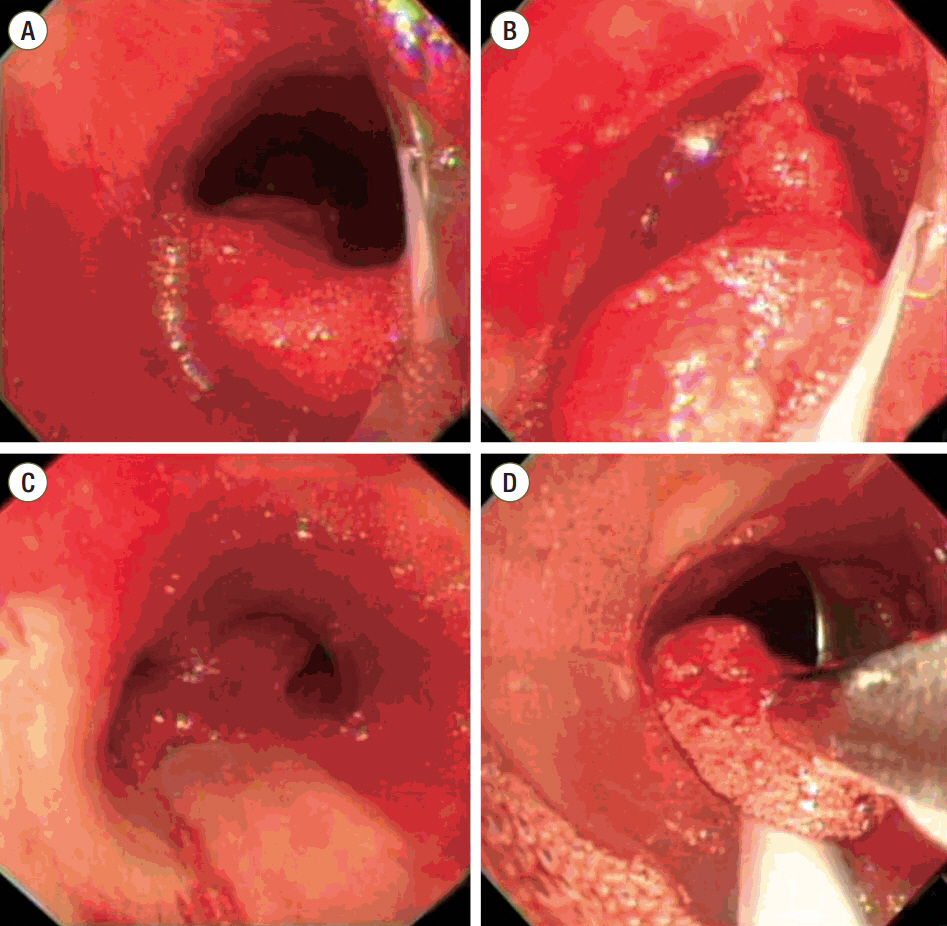
Fig. 2. Bronchoscopy reveals thick blood clots running from the distal trachea (A, B) to the main carina and both bronchi (C). Forceps were used to remove the clots (D).
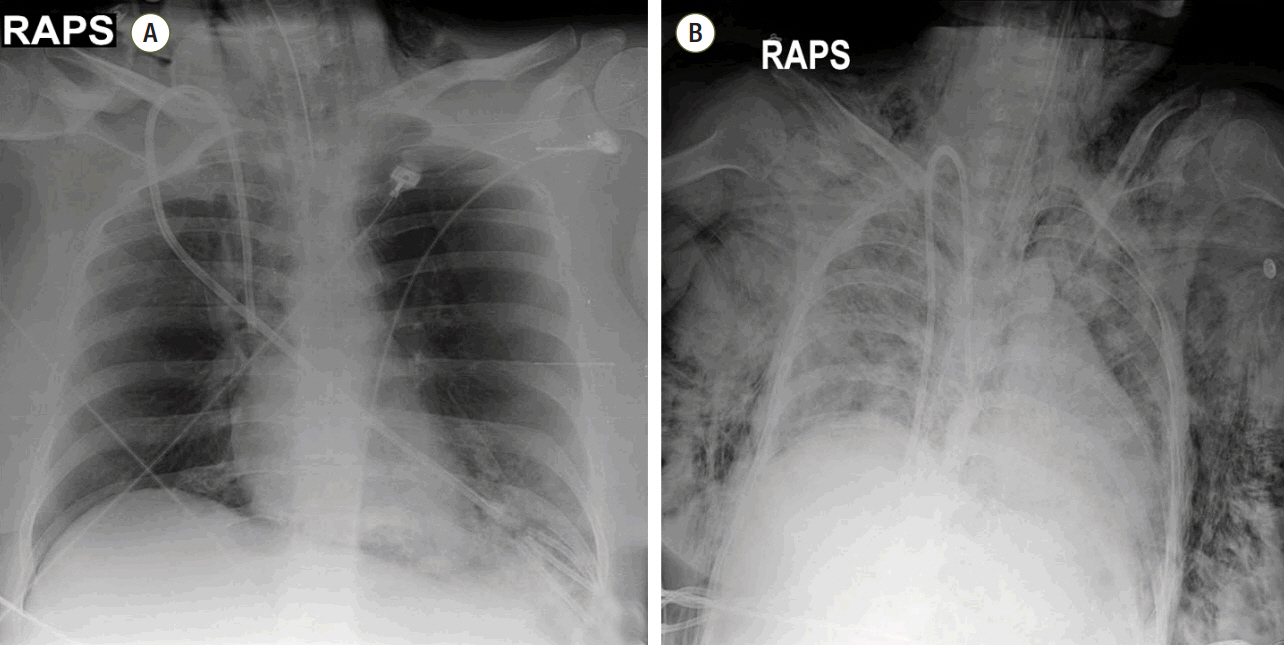
Fig. 3. (A) A post-intubation chest radiograph reveals aggravated atelectasis in the lingular division. (B) Diffuse subcutaneous emphysema is evident in the chest radiograph. RAPS: right anterior posterior supine.
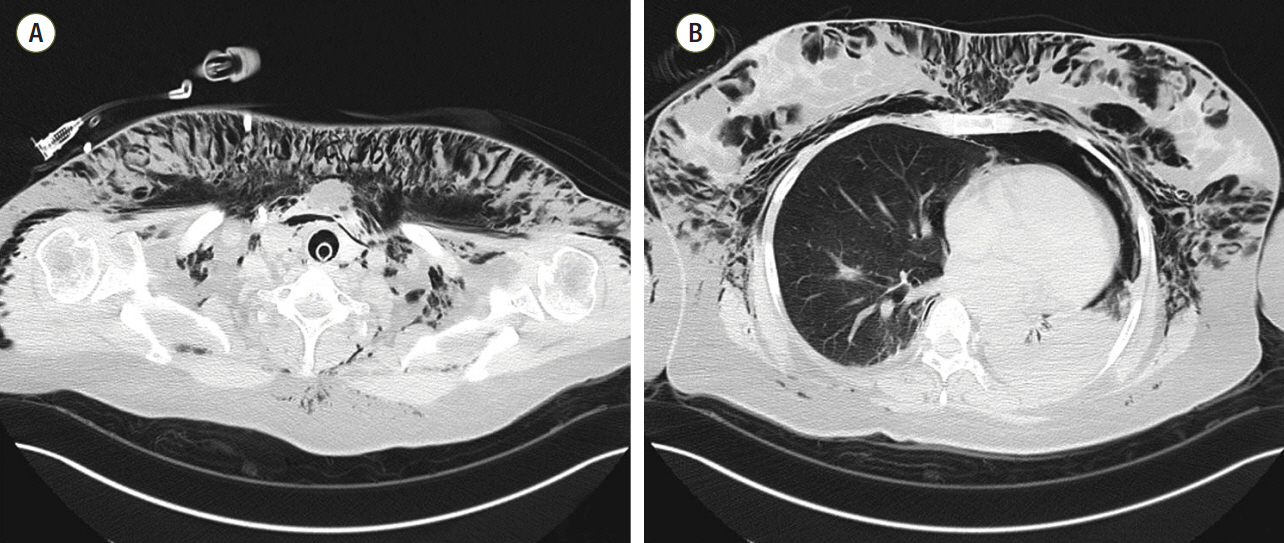
Fig. 4. (A) Chest CT reveals extensive pneumomediastinum and subcutaneous emphysema in both thoraces. (B) Moderate pneumothorax is evident in the left lung. CT: computed tomography.

Fig. 5. Chest radiography reveals improvement of the subcutaneous emphysema and the pneumothorax of the left lung. R: right.
Reference
-
References
1. Ricard JD. Manual ventilation and risk of barotrauma: primum non nocere. Respir Care. 2005; 50:338–9.2. Denehy L. The use of manual hyperinflation in airway clearance. Eur Respir J. 1999; 14:958–65.
Article3. López Rodríguez A, López-Sánchez L, Julía JA. Pneumoperitoneum associated with manual ventilation using a bag-valve device. Acad Emerg Med. 1995; 2:944.4. Kim JB, Jung HJ, Lee JM, Im KS, Kim DJ. Barotrauma developed during intra-hospital transfer -a case report-. Korean J Anesthesiol. 2010; 59 Suppl:S218–21.
Article5. Macklin MT, Macklin CC. Malignant interstitial emphysema of the lungs and mediastinum as an important occult complication in many respiratory diseases and other conditions: an interpretation of the clinical literature in the light of laboratory experiment. Medicine. 1944; 23:281–358.6. Gammon RB, Shin MS, Buchalter SE. Pulmonary barotrauma in mechanical ventilation. Patterns and risk factors. Chest. 1992; 102:568–72.7. Turki M, Young MP, Wagers SS, Bates JH. Peak pressures during manual ventilation. Respir Care. 2005; 50:340–4.8. McCarren B, Chow CM. Manual hyperinflation: a description of the technique. Aust J Physiother. 1996; 42:203–8.
Article9. Windsor HM, Harrison GA, Nicholson TJ. “Bag squeezing”: a physiotherapeutic technique. Med J Aust. 1972; 2:829–32.
Article10. Redfern J, Ellis E, Holmes W. The use of a pressure manometer enhances student physiotherapists’ performance during manual hyperinflation. Aust J Physiother. 2001; 47:121–31.
Article11. Patman S, Jenkins S, Smith K. Manual hyperinflation: consistency and modification of the technique by physiotherapists. Physiother Res Int. 2001; 6:106–17.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Barotrauma developed during intra-hospital transfer: A case report
- Massive Hemoptysis Cases Intubated with the Univent(R) Bronchial Blocker for Lung Protection
- A Case of Pneumoperitoneum After Mechanical Ventilation in A Child with Severe Bronchial Asthma
- Double-lumen Endotracheal Tube in the Management of Massive hemoptysis
- A Case of Massive Hemoptysis due to Dieulafoy's Disease of the Bronchus
