Delayed Intracerebral Hemorrhage from a Pseudoaneurysm Following a Depressed Skull Fracture
- Affiliations
-
- 1Department of Neurosurgery, RUSH University Medical Center, Chicago, IL-60612, USA. manish_kasliwal@rush.edu
- 2Department of Radiology, RUSH University Medical Center, Chicago, IL-60612, USA.
- KMID: 2155718
- DOI: http://doi.org/10.5469/neuroint.2016.11.1.42
Abstract
- A 26-year-old male presented with delayed intracerebral hemorrhage from a ruptured distal middle cerebral artery pseudoaneurysm that followed a compound depressed skull fracture from years ago. The brain protrusion through the skull defect likely resulted in stretching and subsequent tearing of the arterial wall resulting in the pseudoaneurysm formation. No prior report of such a clinical occurrence exists in the literature. We highlight an unusual but treatable cause for intracerebral hemorrhage following surgery for traumatic brain injury.
Keyword
MeSH Terms
Figure
-
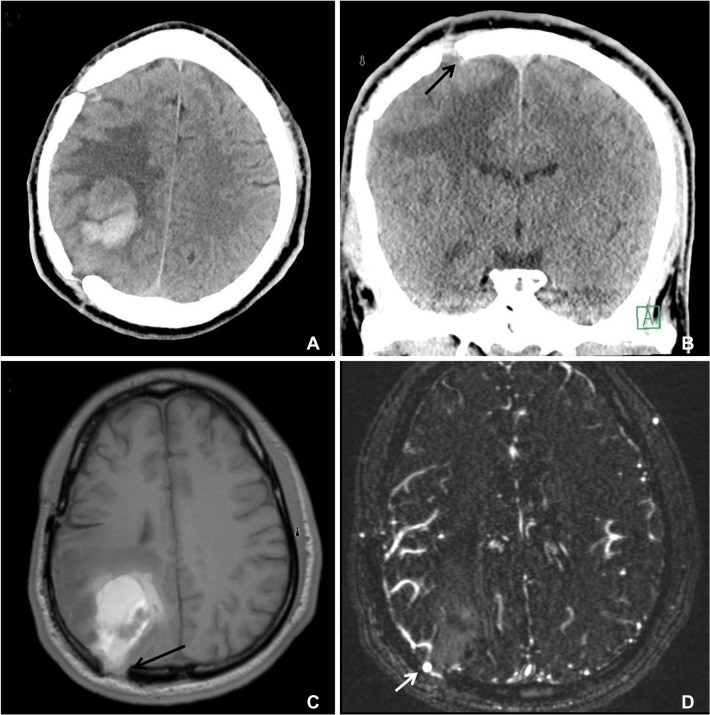
Fig. 1 Axial non contrast CT scan of the head (A and B) and MRI (C) showing a 3.5 × 2.6 cm acute intraparenchymal hematoma in the right parietal lobe along with a large defect in the cranium in the parietotemporal region from prior craniotomy. An old, right parietal craniotomy is redemonstrated. Also visible is the protrusion of the brain parenchyma through the defect (arrows in the B and C), particularly along its superior aspect seen both on CT and axial MRI. An axial MRA image (D), suggestive of a pseudoaneurysm (arrow).
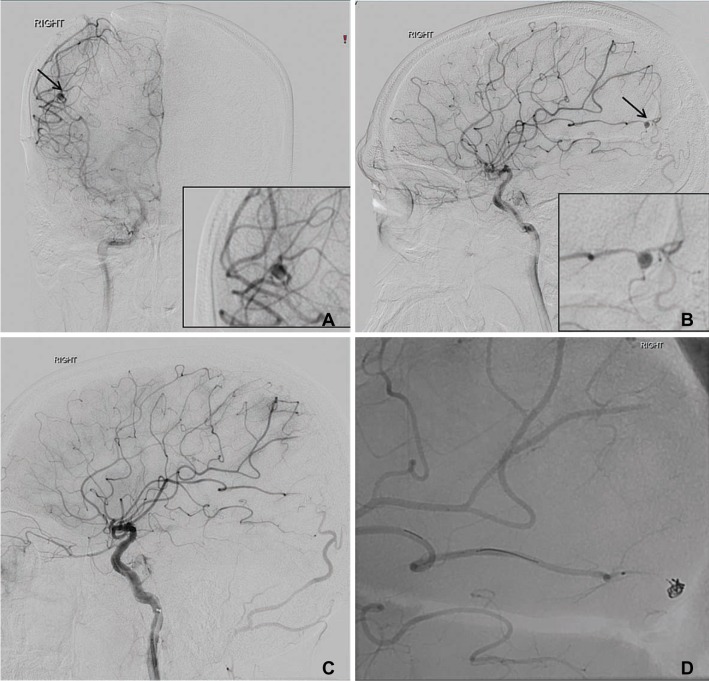
Fig. 2 AP (A) and lateral (B) views of conventional angiograms following injection of the right-sided internal carotid artery, showing the pseudoaneurysm (arrows) arising from the right middle cerebral artery M4 segment, measuring 3×3 mm in size with a neck of 1 mm (2A and B, middle image) that was successfully coiled (2C). Insets in 2A and B show a magnified view of the aneurysm. An unsubtracted lateral view (D) of the angiogram showing coil mass occluding the aneurysm.
Reference
-
1. Bullock MR, Chesnut R, Ghajar J, Gordon D, Hartl R, Newell DW, et al. Surgical management of depressed cranial fractures. Neurosurgery. 2006; 58:S56–S60. PMID: 16540744.
Article2. Prasad GL, Gupta DK, Mahapatra AK, Borkar SA, Sharma BS. Surgical results of growing skull fractures in children: a single centre study of 43 cases. Childs Nerv Syst. 2015; 31:269–277. PMID: 25227164.
Article3. Ohta M, Matsuno H. Proximal M2 false aneurysm after head trauma--Case report. Neurol Med Chir (Tokyo). 2001; 41:131–134. PMID: 11372556.4. Yi HJ, Kim KM, Ko Y, Kim YS, Oh SJ, Oh SH. A spontaneous giant pseudoaneurysm presenting with chronic headache in adolescent. Childs Nerv Syst. 2006; 22:295–299. PMID: 16496160.
Article5. Voelker JL, Ortiz O. Delayed deterioration after head trauma due to traumatic aneurysm. W V Med J. 1997; 93:317–319. PMID: 9439194.6. Larson PS, Reisner A, Morassutti DJ, Abdulhadi B, Harpring JE. Traumatic intracranial aneurysms. Neurosurg Focus. 2000; 8:e4. PMID: 16906700.
Article7. Komiyama M, Morikawa T, Nakajima H, Yasui T, Kan M. "Early" apoplexy due to traumatic intracranial aneurysm--case report. Neurol Med Chir (Tokyo). 2001; 41:264–270. PMID: 11396307.8. Miley JT, Rodriguez GJ, Qureshi AI. Traumatic Intracranial Aneurysm Formation following Closed Head Injury. J Vasc Interv Neurol. 2008; 1:79–82. PMID: 22518228.9. Fleischer AS, Patton JM, Tindall GT. Cerebral aneurysms of traumatic origin. Surg Neurol. 1975; 4:233–239. PMID: 1162596.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Spontaneous Elevation of Neonatal Depressed Skull Fracture
- Elevation of Depressed Skull Fracture with a Cup of Breast Pump and a Suction Generator: A Case Report in Technical Aspects
- Skull Perforation and Depressed Fracture Following Skull Fixation for Stereotactic Surgery
- Angiographically Progressive Change of Traumatic Pseudoaneurysm Arising from the Middle Meningeal Artery
- Traumatic Intracerebral and Subarachnoid Hemorrhage Due to a Ruptured Pseudoaneurysm of Middle Meningeal Artery Accompanied by a Medial Sphenoid Wing Dural Arteriovenous Fistula
